Every year TGEU (Transgender Europe) releases an index of key indicators on trans rights, along with a map highlighting the performance across the continent (Europe and Central Asia).
The 2020 map, indicator and key stats are available here.
Frustratingly, in spite of requests for inclusion, there is still no analysis specific to trans children’s rights across Europe..
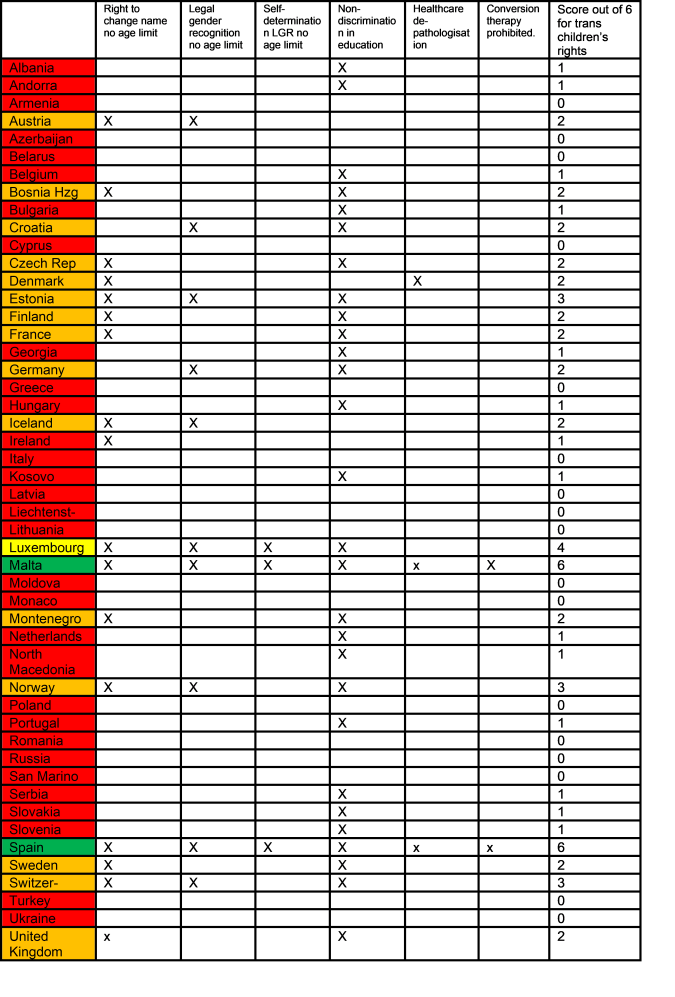
Taking the TGEU data, I’ve selected the six indicators that relate specifically to trans children, and highlighted the performance across the continent. These relate to the areas of Legal Recognition (3 indicators), Health (2 indicators) and Non-Discrimination (1 indicator). These six indicators are the only data collected by TGEU which have relevance for transgender children & young people and provide coverage of basic or fundamental rights.
The results are absolutely shameful.
RED: Actively hostile with little or no fundamental rights for trans children.
63% (31 out of 49 countries) meet 0 or 1 indicators with 9 scoring 0 for failing to provide even the very basics of non discrimination. The country is actively hostile to the very existence of trans children.
AMBER: Rudimentary rights for trans children.
30% (15 countries) meet only a few of the basic rights of trans children (score 2 or 3), These countries are failing trans children. This includes the UK where there is no legal recognition, nor coverage of health indicators, including no anti-conversion therapy legislation, in spite of signposting for government prioritisation following the National LGBT survey of 2018.
YELLOW: Moderate fundamental rights for trans children.
The single country meeting 4 or 5 indicators is Luxembourg, which meets the basics for Legal protection and non discrimination but does not meet either of the indicators for health.
GREEN: Fundamental rights for trans children are met.
Only 4% (two countries), meet all the fundamental rights of trans children and young people with 6 indicators in all three areas. Spain and Malta.
Only 6% (3/49) of European countries have even moderate fundamental rights for transgender children and young people.
We need more people to care about this.
We need rights organisations (Stonewall, Amnesty, TGEU, Save the Children, UNICEF, Plan International) to collect data, and analyse this data, to help us hold government’s to account for the gross failings towards the rights of trans children across Europe. We need TGEU members to start asking TGEU to provide analysis specific to trans children and young people.
The six indicators above are a snapshot, taken from the TGEU 2020 dataset. There are other indicators that could be tracked that would give an even clearer picture of the ways in which Europe fails trans children. We need to start including dis-aggregated data in our analysis on trans rights, dis-aggregation that shows the specific ways in which trans children are failed. We need to start collecting data specific to trans children. We need dis-aggregated analysis of the data that we do have. And we need to start raising our voices about the rights violations that trans children face across Europe and beyond.
Some more UK commentators, and even the Royal College of General Practitioners, have recommended a ‘watchful waiting’ approach for trans children.
I’ve written previously that this UK guidance is out of synch with the medical recommendations in the US, Canada, Spain, New Zealand, Australia. How it is out of synch with experts in other countries who consider watchful waiting, which they more accurately describe as ‘delayed transition’, to be harmful to trans kids.
Here I want to share my own experience, and the experience of other parents, on how watchful waiting plays out in practice. For me watchful waiting is a misleading term – it sounds very benign and sensible. While the term used to describe this elsewhere, ‘delayed transition’, is a more accurate description, the reality for those living through it is that ‘prolonged rejection’ is a better description of what ‘watchful waiting’ means in practice.
From as soon as my child could properly speak, they asserted ‘I am a girl’. For some initial time, in total ignorance about gender diversity, I opted for active rejection: ‘No, you are not a girl you are a boy’.
Months and months of daily (multiple times a day) active rejection followed. My child would insist their gender several times a day. Active rejection was not leading to any change in my child’s insistence (just an increase in my child’s distress and depression). I researched and came across the UK guidance for ‘watchful waiting’, whereby they recommend a supposedly neutral approach where a child is not actively rejected (ie stopping saying ‘no you are not a girl’) but without any active affirmation (without saying, ‘ok we will call you a girl’).
We really tried that watchful waiting approach with our child. This is how it played out in practice with an insistent, consistent, persistent and increasingly distressed trans child (and these are the children who we are talking about, who most obviously benefit from affirmation).
Every single day my child would cry and say ‘I’m a girl’. During watchful waiting we would tell them I loved them and we didn’t need to talk about gender – They were left thinking their mum and dad did not understand or did not care about this thing that was so important to them.
Every day they would cry themselves to sleep saying ‘But I’m a girl’. I would hug them and tell them I loved them, whilst ignoring the thing that was causing their distress. – They were left thinking that one part of them was broken – un-loveable – unacceptable. How shame inducing? How pathologizing?
Every day I would try to actively break down gender stereotypes, try to break down gender roles or restrictions around gender expression without supporting my child’s identity. This only made my child sadder as their mum was missing the point entirely. In one conversation that sticks in my mind:
Child: ‘But mummy I am a girl’
Me: ‘Boys and girls can do all the same things. Would you like a doll?’
Child: ‘I don’t like dolls, I am a girl…. can I have a spiderman’
In another one:
Child: ‘I’m a girl’
Me: (Desperately thinking about what my child might associate as typically ‘girl activities)… Would you like to try out ballet classes?’
Child: ‘I don’t like dancing’
Me: ‘What do you like?’
Child: ‘Climbing trees. Girls can like climbing trees’.
I was not listening to my child. I was rejecting her.
Every day they spent sad, rejected, and fixated on the topic of gender. They were losing out on the carefree fun childhood of their peers. Every day spent sad and depressed and rejected is a lost day of childhood. Every day spent feeling that who they are is unacceptable to their mum, is a day piling on shame, self-hate, low self-esteem.
I watched them get lower, get less happy, get less curious about the world, get less excited about life get sadder, get more isolated and alone. This is what I was watching. What was I waiting for? My child had told me in very consistent, persistent and insistent terms what she needed. She needed to be loved and accepted as a girl. It was the only thing that mattered to her and she felt deeply rejected, deeply broken, deeply unacceptable. Was I waiting for her mental health to crash? Was I waiting for her to snap out of it? Was I waiting for her to reach an arbitrary age? Was I waiting for her to turn 10?
What would waiting until age 8 or age 10 until I stopped passively rejecting her mean for my child? What would be the benefit to her, of keeping her in a state of continued rejection, depression and sadness until age 8 or 10 as the NHS advises?
What are the risks of waiting until age 8 or age 10 until I stop rejecting her?
What is at stake?
For me the biggest stake is her childhood, her happiness, her self-esteem, her self-worth, her curiosity, her interest, her learning, her education. I care about her happiness right here and now.
During our phase of watchful waiting, my child was on pause, she was stuck, she was unable to thrive.
As soon as we moved to affirmation, everything changed.
Affirmation was a much easier thing to do in practice.
She said:
‘I’m a girl’
And we said: ‘ok we will call you a girl’.
We switched pronouns. As far as our family life was concerned, that was a very quick and easy switch. We switched pronouns and our daughter thrived. She has never once cried herself to sleep since that day. She no longer wanted to talk about gender every time we were alone. She started to talk about animals, and space, and nature, and how things work. She started to explore. She started to have a childhood. She became lighter and carefree. A huge burden lifted from her shoulders (and noticeably shifted to ours as we sought to get the wider world to respect her identity).
The price of watchful waiting was very high for my family. The price was very high for my daughter.
Watchful waiting robbed my daughter of a period of her childhood. A period when she could have been happy and loved and accepted and carefree. When instead she was left feeling rejected and broken. For a child like mine, watchful waiting causes harm.
I am thankful that we had access to other sources of information (my next blog will be on the evidence base for affirmation versus watchful waiting).
I am thankful that the period of rejection was not so long, and that the damage to her self-esteem was not deep.
I am thankful that since the day we stopped rejecting her, the simple change of pronoun, she has flourished in every way.
She laughs, she can dream, she can learn, she can play. She is having a carefree happy childhood. This was literally not possible under prolonged rejection (ie watchful waiting).
Many other parents tell the same story. Of trying watchful waiting for months or years and watching their child sink.
People with no experience of living daily with trans kids need to start listening to the impact ‘watchful waiting’ has in practice. They need to start listening and understand that it is neither neutral, nor benign, nor easy. It is hard to passively reject your child daily. It is hard to watch them sink. It is an approach that fundamentally misunderstands insistent, consistent, persistent trans children. It is an approach that fundamentally undervalues the right of a trans child to a happy childhood.
Trans kids only get one childhood. They need to know they are loved as who they are. They need to know their parents and carers have their backs, will listen to them, will accept them, will stand up for them.
Stop rejecting trans kids. Passive rejection can hurt as much as active rejection. Quiet rejection, rejection through silence and omission can hurt as much as loud rejection.
Transgender trend ‘School resource pack’ – A teacher’s perspective –
The writer has more than 12 years experience in teaching, including head of year in secondary and within a SEND setting.
As a teacher my first question is who has written this?
Who are the authors?
Usually on resources you see a whole load of signatories, accreditation and endorsing organisations. Here there’s nothing.
How am I meant to use it?
It is not a resource pack (it contains no specific resources) and I can see no practical application for it.
Looking at the linked website, ‘about us section’, the organisation claims to be founded by a group of parents who have created a website and twitter account but have no other stated organisation purpose or role which gives them legitimacy.
The website ‘founder’s’ primary previous job experience is being an ‘accredited communication skills trainer’ (read bullshitter?).
She mentions she founded a school and worked in various roles in the classroom and playground. This implies she is unqualified (if she was a trained teacher or head, or worked as governor, she would surely have mentioned that).
Reading more of her blurb it quickly links to a website full of naff stock photos and seems to be motivated to sell a book, which seems to be self-published.
Doing a cursory nose around the website’s FAQ section, the first FAQ they have chosen to address is very telling:
Aren’t you just transphobic?
No, we believe that transgender people deserve the same civil and human rights as all of us and should not face discrimination. As the term ‘phobic’ literally means ‘irrational fear’ we want to make it very clear that we are not afraid of, or prejudiced against, transgender people in any way.
Given the amount of prejudice content they are pedalling this answer is an immediate red flag.
It’s a bit like a organisation’s website (which is full of material that advocates racism) including a headline FAQ of : “Aren’t you racist?” Happily responding with – ‘No I’m not racist because racism actually means this’.
On to the publication in question
Despite being formatted like an official guidance document, the prejudice and agenda which came through from a brief look of the website are easy to spot.
The document starts by stating that it was developed in partnership with teachers and child welfare staff, again this is tellingly unspecific.
In these days of academies and free schools employing staff without specialised training to teach, the term ‘teacher’ has lost some of its protected status, and anybody who works in a school during the day from cleaners to ICT technicians has to attend child protection training about prioritising welfare. So you can see how they might have stretched some meagre credentials. Critically, it doesn’t state ‘welfare professional’ or name any specific roles such as ‘Head of Year’ or ‘Safeguarding Lead’
The introduction sets out its goal to “Manage the (se) issues” of official transgender schools guidelines.
The following content on Page 5 titled “why is it needed” is clearly anti-transgender rights and is scaremongering.
It is full of sensationalist soundbites equating gender non-conformity with sexual orientation, highlighting increases in referrals to gender clinics, and even implying that the internet is not to be trusted as it causes something they name ‘rapid onset gender dysphoria’ (thank goodness for Net Neutrality eh).
I almost give up at this point, I am not going to be reading their list of fallacies or ‘case studies’.
Both the title and details of the section ‘Transgender, gay, lesbian, ASD or troubled teenager?’is very offensive not least to children who have suffered abuse or who have ASD.
As schools we have been tasked by the DfE to promote fundamental British Values of:
The rule of law.
Individual liberty.
Mutual respect for and tolerance of those with different faiths and beliefs.
I don’t see how this document can fit within these modern values.
I see no way that schools would touch this publication with a barge-pole.
Schools are time and money poor, therefore no one will have the time to read it, or the money to print it.
The priority of school leaders is the safety of young people and ensuring that they make progress.
For teachers this means reporting concerns on to the correct person and spending hours preparing lessons, marking and reporting data.
This document includes bad, unsupported, advice coming from a website with a clear agenda of prejudice against the children it claims to support. Reading it is a waste of teacher’s time.
Scotland is currently holding a consultation on reforming their Gender Recognition Act. This proposes options to simplify the process for transgender people in Scotland to obtain full legal gender recognition (acquiring a Gender Recognition Certificate and amending their birth certificate).
This consultation seeks views on reforming the 2004 Act. The Scottish Government proposes to streamline the process for obtaining legal recognition and also to allow people aged 16 and over to apply. We are also seeking views about the options for people under 16 and for recognition of non-binary people.
The consultation provides key information on the Gender Recognition Act. It is critical to note however that even without a Gender Recognition Certificate, transgender people are legally protected under the 2010 Equality Act and have rights to change identity markers in systems including schools, the NHS and their passports, and have the right to use facilities matching gender identity. The Gender Recognition Act is however the only route to updating a birth certificate.
“GRC” – a gender recognition certificate. Under the 2004 Act, a full GRC provides legal recognition of an applicant’s acquired gender. When a GRC is issued under the 2004 Act, the applicant’s legal sex also changes to male or female. ”
“The 2004 Act allows transgender people aged 18 and over to apply for legal recognition of their acquired gender and to change their legal sex accordingly”
The consultation considers two main models for gender recognition, the current system of an assessment model (where a doctor, psychologist and or court ‘evidences’ a person’s gender identity) or a self-declaration model (as already applied in Norway, Denmark, Malta, Colombia, Argentina, and the Republic of Ireland).
For an example of how this is working in practice, this article provides a useful overview of how a self-declaration based process is already in action in the Republic of Ireland.
I won’t focus here on the proposed options for how the gender recognition system will operate, but will instead give attention to eligibility based on age – namely whether trans youth and trans children are permitted to get a Gender Recognition Certificate and change their birth certificate.
Under 18s.
At present in Scotland, as elsewhere in the UK, trans youth and trans children under 18 are not eligible for a Gender Recognition Certificate, meaning under 18s cannot update their birth certificate. Trans children and youth are however given legal protections under the 2010 Equality Act, and already have the right to change their gender marker in almost all other documentation, without the need for a Gender Recognition Certificate (including a right to change their gender marker in their passport, and in systems including schools and the NHS) (*as with adults options for identity recognition for trans youth/children with non-binary identities are extremely limited).
The consultation questions:
The survey starts with 4 questions for how GRC should work for adults including:
Question 1 The Scottish Government proposes to bring forward legislation to introduce a self-declaratory system for legal gender recognition instead. Do you agree or disagree with this proposal?
16-17 year olds.
The consultation proceeds to focus on 16-17 year olds:
“The Scottish Government considers that people aged 16 or older should be able to apply for legal recognition of their acquired gender using the proposed self-declaration process.
4.05. There is clear evidence that people aged 16 do live full time in their acquired gender and want this to be legally recognised. For example, the Women and Equalities Select Committee heard evidence from LGBT Youth Scotland to this effect. In the Republic of Ireland, 8 people aged 16 and 17 have received a GRC31 after obtaining a court order permitting them to apply under their self-declaration system. The court in the Republic of Ireland is required to consider evidence about the young person’s transition to their acquired gender. ”
Question 5 The Scottish Government proposes that people aged 16 and 17 should be able to apply for and obtain legal recognition of their acquired gender. Do you agree or disagree?
It is curious that the report notes the “clear evidence that people aged 16 do live full time in their acquired gender and want this to be legally recognised” and yet in subsequent sections does not similarly note the existence of transgender children under the age of 16. Parents of transgender children, and other groups supporting transgender young people were perhaps overlooked in the preparatory consultations? This oversight makes it especially important that parents and supporters of transgender children and young people provide feedback during this consultation that transgender children do indeed exist, and those under the age of 16 both want and need full legal recognition. Inputs from any under transgender young people themselves might also be an important addition to this consultation.
Under 16s
The consultation moves on to consider under 16s:
“4.08. The Scottish Government’s view is that there is a careful balance to be struck in relation to people under 16. On the one hand, we should treat children with dignity and respect, giving weight to their views and wishes in line with their individual capacity. On the other hand, we should ensure that children have the right protection and care. 4.09. People who are under 16 years of age can act on their own behalf in relation to a range of matters. Annex E contains further information about this. The CRWIA at Annex M refers to research evidence about children who identify as transgender. 4.10. The Scottish Government considers that there are five broad options in relation to people under 16 being able to apply for legal gender recognition.”
The consultation proceeds to outline 5 potential options for transgender children under the age of 16. I’ve quoted these here in full, following which I’ve outlined my thoughts on each option:
Under 16s – option 1 – nothing for those under 16
4.11. Under this option, applicants would have to be at least 16 to apply for legal recognition of their acquired gender. This would be straightforward, but would stop those under 16 with a clear view of their gender identity from obtaining legal gender recognition.
Under 16s – option 2 – court process
4.12. Option 2 would be for Scotland to adopt a court based process.
4.14. Any court based process, whether instigated by a child’s parents or by the child themself, would focus on the assessment of the child’s welfare. We would also consider specifying the matters the court would have to have regard to in determining what was in the child’s best interests. 4.15. Under this option, a court action could be raised by the child if they had sufficient capacity to do so, or if they did not, by a person or persons who had PRRs (parental responsibilities and rights) for them acting on their behalf.
4.19. Malta has a court based process of legal gender recognition for those under 18. Those with parental authority for a child may file an application in the court. The court must consider the best interests of the child and give due weight to the views of the child depending on their age and maturity
4.20. In the Republic of Ireland, applications cannot be made by those aged under 16. However, applications by 16 and 17 year olds require to be accompanied by a court order permitting the application to be made. The court may only grant the order if the child’s parents, surviving parent or guardian consents. Two medical certificates must also be produced to the court. The medical certificates must confirm that: · the child has a sufficient degree of maturity to decide to apply for gender recognition; · the child is aware of, has considered and fully understands, the consequences of that decision; · the child’s decision is freely and independently made; and · the child has transitioned, or is transitioning to, their preferred gender.
4.21. Under option 2, a child who may not have reached puberty might apply to the court or a person with PRRs for such a child might apply.
Under 16s – option 3 – parental application
4.22. Option 3 would be to permit an application to be made on behalf of a person under 16 by someone with PRRs (parental responsibilities and rights) for them. Typically, this would be the child’s parents. Further information about PRRs, when parents get them and who else may have PRRs is in Annex F. 4.23. Usually, where more than one person has parental rights in relation to a child, each can exercise their rights without the consent of the other or any of the others.36 4.24. Where a person with PRRs is reaching a major decision regarding the fulfilling or exercise of PRRs, the person is under a duty to have regard to any views the child expresses, taking account of the child’s age and maturity. The person making the decision must also have regard to any views expressed by any other person with PRRs for the child concerned.37 The Scottish Government considers that seeking legal recognition in an acquired gender is an example of a major decision. 4.25. One possibility under this option would be to require the application to be made by all parents with PRRs for a child. This would mean that a person who had PRRs for the child but was not their parent would not require to be involved. However, we would still expect the person(s) applying on the child’s behalf to have regard to the views of such a person. 4.26. Another possibility under this option would be to require all people with PRRs to apply, not just a parent or parents with PRRs. This may mean that a local authority that had PRRs for a child would need to be involved in the application process. 4.27. If all the people who required to be involved in the application did not agree38, then a court order could be sought under existing arrangements. Section 11(1) of the Children (Scotland) Act 1995 allows the Sheriff Court or the Court of Session to make an order in relation to PRRs. The court could then make a decision based on the child’s welfare. 4.28. There are some children for whom no one has PRRs. One option might be for a person who has an interest to obtain PRRs from the court and then apply for legal gender recognition on behalf of the child.
4.30. In summary, therefore, under this option all parents with PRRs (or, perhaps, everybody with PRRs) would have to apply, having had regard to the child’s views. If there is a dispute amongst those with PRRs, an application could be made to the court to resolve the matter. There may be restrictions on the role of a person with limited PRRs. 4.31. Under this option, applications could be made on behalf of very young children, including both those who lack legal capacity and who have not reached puberty.
Under 16s – option 4 – minimum age of 12
4.32. Option 4 would permit children aged 12 and above to apply in the same way as those aged 16 or above
4.34. However, this option would take no account of a child’s capacity to take decisions nor their physical maturity.
4.36. The Scottish Government does not favour this option as it would allow a child to apply irrespective of their capacity to understand the nature and consequences of their decision.
Under 16s – option 5 – application by capable child
4.37. Option 5 would permit a person under 16 to apply in the same manner as an adult, provided they had capacity to understand the consequences of recognition in their acquired gender.
4.38. Under this option, someone would have to test the child’s capacity. This could potentially be done, for example, by a registered medical practitioner, or by a practising solicitor.
4.40. A person under 16 has legal capacity to instruct a solicitor, in connection with any civil matter, where the person has a general understanding of what it means to do so. Someone aged 12 or more is presumed to be old and mature enough to have such understanding.
The section ends with question number 6, which asks consultation respondents to state which of the 5 potential options for transgender children under 16 they most favour.
Question 6
Which of the identified options for children under 16 do you most favour? Please select only one answer.
option 1 – nothing for those under 16
option 2 – court process
option 3 – parental application
option 4 – minimum age of 12
option 5 – application by capable child
My response to the consultation
My initial thoughts to the above is as follows:
Option 1 – nothing for under 16s, is unacceptable. Many of our trans children are living as their identified gender from primary school, including changing their gender marker in other systems including on their passport. Why then should they have to wait until 16 to have who they are fully recognised in law? When they have been living for years with a passport and other markers in their gender identity, why should their birth certificate be out of sync? Inability to update birth certificate adds to stress for trans children that their identity will be unwillingly disclosed and presents to them the reality that the state does not fully respect them until adulthood. Trans children exist, and waiting until 16 or 18 for proper legal recognition is denial of basic rights for these young citizens.
Denying rights to under 16s is at odds with the recent WPATH (World Professional Association for Transgender Health) statement on identity:
“WPATH advocates that appropriate gender recognition should be available to transgender youth, including those who are under the age of majority,”
Option 2 – court process seems like an expensive, bureaucratic, stressful and unneccessary requirement. I would like to learn more from Ireland, who has a similar requirement for 16-17 year olds which is currently under review. Australia, which has just got rid of a requirement for trans youth to go to court for hormone treatment, provides a useful case study of this process.
CASE STUDY: Australian experience of a court based process
Australia until very recently required under 16s to go to court to gain approval for gender related medical care. Families and transgender children in Australia found the process of going to court stressful and upsetting. When one family were told that the requirement to go to court was being removed, one family reportedly “were unable to contain their tears of relief” with their child commenting “No longer will young transgender young people have to keep justifying who they were“.
World leading specialist in supporting transgender children, Dr Telfer, Director of the Gender Service at the Royal Children’s Hospital in Melbourne described the amount of time gender specialists were having to devote to guiding families through the court proceedings:
“Gender Clinic staff have had to spend considerable time on counselling families on what the court process would be like, Dr Telfer said.
“No-one wants to be in a courtroom. Usually it’s a place where you go when something is wrong.
The requirement for transgender youth to go to court was described as “costly, traumatic and unnecessary”.
The director of legal advocacy at the Human Rights Law Centre, Anna Brown, described the decision to stop forcing transgender children in Australia to go to court as a “stunning victory” for young transgender people.
“This will make a profound difference to the lives of many young trans people who will now be relieved of the burden of a costly and unnecessary court process”
“This bizarre legal anomaly was born of outdated attitudes to trans young people”
“Importantly, also, for the young people themselves, going to court can be hugely taxing,”
“This decision is a huge victory for so many young people and their families. The latest research shows that there are probably around 45,000 trans and gender-diverse young people in Australia, and this will save them enormous amounts of money, time and heartache.”
Australia has made the decision to move away from requiring transgender children to go to court. Why then would Scotland wish to impose this on Scottish trans children? Based upon the Australian experience, the Option 2 court process, is not the right decision for our children.
Option 3 – parental application seems instinctively a sensible option. With parental approval children like my daughter could get their identities fully legally recognised. This would however limit options for youth who do not have parental support, and such youth would either need to wait until 16 or would need to have recourse to an alternative option eg to the court option. I wonder whether there are many youth without any parental support for whom gaining a GRC pre 16 would be a major priority? I’d welcome feedback from trans youth or organisations working with trans youth.
Option 4 – minimum age of 12 is largely ruled out by the Scottish consultation, and I would agree that basing declaration on age, rather than capacity for decision-making, would be unworkable.
Option 5 – application by capable child is attractive in theory but I question how it would work in practice. It would require an administration layer including professional gate keepers, requiring our children to submit to an assessment, and I wonder who would be willing to test a child’s capacity for this purpose. This might result in a very small number of medicalised gate-keepers and subject to waiting lists, delays and arbitrary protocols. There’s also a very serious question about how to ensure such professional are able to assess a child’s capacity in a sensitive and appropriate manner – those of us with trans children are well aware of the level of transphobia and ignorance about trans children so common across the UK.
Seeking another opinion
I decided to reach out to the Scottish Trans Alliance who provided their view on the options for under 16s
Scottish Trans Alliance:
“We’re currently in favour of Option 3 – the ‘parental application‘ option – where under 16s would be allowed to change gender on birth certificate on submission of a simple statutory declaration with signed parental consent. This would mirror how name changes on official documents are already done for under 16s.
We think that if a young trans person under 16 has unsupportive parents then the most urgent problems they will be facing are likely to be whether they are safe from transphobic emotional abuse at home and whether they are able to wear clothes they want and use the verbal pronouns they want. We think that it is rare that a child under 16 with unsupportive parents will be in a confident and safe enough position to risk trying to change their birth certificate against the wishes of their parents.
We think that nearly all under 16s who have been able to successfully start living fully in their gender identity (and therefore are at the point where it would make sense to change their birth certificate to improve their privacy) will have at least one supportive parent. However, it is important that there is a way of ensuring that an unsupportive parent is not able to block the wishes of the young person and their supportive parent. If a court process is needed to resolve a family dispute about whether a young person should be granted a GRC, then we think the court ought to be obliged to uphold the wishes of the young person provided they have capacity to understand the consequences of legal gender recognition.
While Option 5 – the ‘application by capable child’ option – sounds on the surface like a more empowering option than parental application, we have concerns that it may lead to problematic gatekeeping by doctors/solicitors who could be scared to approve the capacity of individual trans young people. It could result in say a 13 year old with supportive parents having to try to prove their capacity to a trans-ignorant doctor only to be told they are too young to understand the consequences and that they have to wait as their parent can’t give consent on their behalf. That could be a very stressful and disempowering experience.
Not allowing under 16s to change the gender on their birth certificate leaves them at risk of schools not taking their gender identity and right to privacy of their gender history seriously. Under 16s usually don’t have bank accounts or many letters sent to them so proving their identity without showing a birth certificate is harder for under 16s than for trans adults. This means trans people under 16 are at greater risk than adults of privacy violation, and transphobic harassment as a result, due to their birth certificate outing them as trans. The intensity of media hostility and resulting negative social attitudes towards trans youth and their families makes privacy rights particularly essential.
Changing birth certificate would have no impact on ability to access hormone blockers but could make a life enhancing difference to moving to a new school without being outed.
It’s worth noting that parents of trans young people under 16 can already change their child’s gender on their passport and medical records so it makes sense to bring birth certificates into alignment with these other official documents.”
Preferred option
Having reviewed the proposed options, and consulted with other stakeholders, the best option for under 16s seems to be Option 3 – parental application.
Flawed research evidence underpinning the consultation
Before concluding, I would also like to share my views on the annexes to the consultation which contain some worryingly flawed ‘evidence’ that if accepted as presented could seriously undermine trans children’s rights.
The Scottish consultation document presents ‘research evidence’ on transgender children in annex M part 4.
ANNEX M: PARTIAL CHILD RIGHTS AND WELLBEING IMPACT ASSESSMENT
What research evidence is available?
4.1 There is evidence that children can experience incongruence between their assigned gender and their gender identity early in life. One study indicates the average age was 8.
4.2 There is a limited evidence base about whether children will continue to experience these feelings in the longer term. Follow-up studies indicate overall that for 85.2% of the children, their distress discontinued either before or early in puberty. 8 However, the rates in the individual studies varied widely. For instance, a 2008 study indicated that in 39% of children the feelings did continue beyond the onset of puberty9 whereas older studies from before 2000 had very much lower rates for children continuing to experience distress after the onset of puberty. It is thought that pre-2000 studies have included children who would not now be considered to be experiencing gender dysphoria. The studies may also be affected by the small clinical population of children with gender dysphoria – studies looking at whether gender dysphoric feelings persisted had a total population of 317 people.
Part 4.2 in particular misrepresents the current body of evidence and is danger of undermining the Scottish consultation through establishing a prejudicial approach to children gaining legal recognition.
It refers to two deeply flawed studies:
Ristori, J and Steensma T.D “Gender dysphoria in childhood” in International Review of Psychiatry, Gender dysphoria and gender incongruence, Vol 28, 2016 Issue 1.
Wallien and Cohen-Kettenis “Psychosexual outcome of gender-dysphoric children” Journal of the American Academy of Child and Adolescent Psychiatry, 47, 1413–1423
We have previously addressed and demonstrated the lack of credibility of these exact studies here.
Conversely, new evidence, that has not been presented in the consultation Annex, suggests a very significantly higher rate of transgender children continuing to identify as transgender as adults and has been reviewed by us here.
4.3 There is also evidence that the more extreme a child’s gender dysphoria was before puberty, the less likely it was that their feelings will recede with the onset of puberty. For those who have reached puberty and continue to experience distress, evidence indicates that their distress then tends to intensify and that depression or self-harming behaviours are also more common in ages 12 and over. It is understood that physical changes caused by puberty may intensify the levels of distress experienced.
4.4 Available evidence suggests that factors arising around the ages of 10 to 13 may help explain changes in how a child feels about their gender: · the changes in social roles between boys and girls as their gender role become more distinct; · the anticipation or experience of physical changes as a result of puberty; and · their first experience of experiencing falling in love and discovering their sexual identity.
4.5. Evidence indicates that there is a difference of experience between boys and girls. 13 Although more boys are referred to gender identity clinics, some studies suggest that gender dysphoria is more prominent in girls.
Part 4.4 relies on one specific flawed study that absolutely does not evidence the claim presented here.
“Steensma T.D et al (2011) “Desisting and persisting gender dysphoria after childhood; A qualitative follow up study” Clinical Child Psychology and Psychiatry Vol16 issue 4”
There is no evidence in this single referenced study that a transgender child changes identity between the ages of 10 and 13 as misrepresented here. This is grossly misleading and risks undermining support for trans children in Scotland gaining legal recognition. We have previously discussed the flaws of this specific paper in some detail here.
4.6 There is evidence that transgender young people are more than twice as likely as non-trans people to be diagnosed with depression (50.6% compared to 20.6%14) and with anxiety (26.7% compared to 10%). There is evidence that this most likely arises due to their experience of discrimination, lack of acceptance, and the abuse they may face and is not an inherent feature of their being transgender. 15 There is also evidence that transition to living in their preferred gender and being supported with gender confirming medical interventions may help improve mental health, in many cases reaching levels experienced in the general population.
It is clear that discrimination and lack of acceptance is damaging to trans youth. The government has a responsibility to tackle this, including through enabling trans children like my daughter to gain full legal recognition. Not allowing full legal recognition to children also sends out a damaging signal to those children and to wider society that transgender children are not worthy of respect or rights.
4.7 Scottish Government officials met members of LGBT Youth Scotland groups aged 13 and over. Their view was that legal gender recognition must be made available to people younger than 16. A person should be able to transition and live in their acquired gender before they have to take their qualifications or go to university. They felt that this would better support their rights not to be discriminated against, for example, at school. A high proportion expressed the desire for their parents (or other people with responsibility for them) to be involved and supporting them through the recognition process.
4.8 LGBT Youth Scotland gave evidence to the Women and Equality Select Committee inquiry into Transgender Equality which setting out the views of transgender people aged under 1817 about the benefits of legal gender recognition in terms of reducing discrimination and improving their mental health.
There is a concerted effort in the UK, as elsewhere, to deny transgender people basic human rights. This campaign is particularly targeting transgender children, the most vulnerable of transgender people, and those with the least power and voice. It is critical that this consultation focuses on listening to transgender children and to those families who support them. Trans children are a small and very marginalised group, and their voices must not get lost in the wider consultation. It is not acceptable to tell transgender children that they have to wait until they are adults before they can be recognised in law.
Appendix A TRANSGENDER CHILDREN – EVIDENCE OF NUMBERS EXPERIENCING GENDER DYSPHORIA OR DISCOMFORT WITH THEIR ASSIGNED GENDER
Appendix A presents a confused view of the difference between transgender children, and children who are gender non-conforming. It alarmingly includes reference to studies from the discredited Zucker, and makes multiple references to “opposite sex behaviour”. It is worrying that a public consultation on gender recognition should have included such a muddled understanding.
Conclusion
Transgender children are one of the most marginalised, voiceless and powerless groups in society. I encourage all who care for transgender children to complete this consultation, and for question 6 I recommend selecting Option C – parental application.
Additionally, in the accompanying comments box for the consultation it would be useful to mention some basic facts:
a) transgender children exist
b) transgender children have legal rights and need legal recognition
c) transgender children face enough challenges, discrimination and hostility already – legal recognition should not be an additional burden for them
The consultation documents mention the “clear evidence that people aged 16 do live full time in their acquired gender and want this to be legally recognised” and yet are silent on on the existence of transgender children or their desire and need for full legal recognition under the age of 16 year.
This right, if enabled, would not be pursued by every transgender child. Parents would not take this option on a whim. This option would be most appropriate for transgender children who have already been living in their identified gender for many years, who likely already have all other identity documents including their passport updated to their identified gender. To deny these children full legal recognition until 16 is a gross betrayal of their rights.
Yet transgender children are one of the least powerful and most marginalised groups in our society. We know that transphobic groups are actively campaigning against the provision of rights to transgender children. The needs and the voices of transgender children may not be heard in this consultation.
It is vital that families of transgender children feed in to this consultation, including those outside of Scotland, making it clear that transgender children do indeed exist and do deserve full legal recognition. Inputs from transgender adults and allies who care for transgender children will also be critical, as supportive families of transgender children are already overwhelmed with the barriers we have to overcome to enable our children to get the rights and the protections that other children take for granted.
Input from any transgender children and young people who are willing to share their thoughts and words would be especially valuable, perhaps explaining what an updated birth certificate would mean to them, or how they feel about being denied the right to full legal recognition.
The consultation can be completed here. It closes on March 1st 2018
“All bullying, including homophobic, biphobic and transphobic bullying causes profound damage, leading to higher levels of mental health disorders,self-harm, depression and suicide.
Central to Christian theology is the truth that every single one of us is made in the image of God. Every one of us is loved unconditionally by God.
Church of England schools offer a community where everyone is a person known and loved by God, supported to know their intrinsic value. This guidance helps schools to offer the Christian message of love, joy and the celebration of our humanity without exception or exclusion.
Church schools must do all they can to ensure that all children, particularly those who may identify as, or are perceived to be, gay, lesbian, bisexual or transgender are kept safe and can flourish.”
A number of Christian commentators have responded with opinion pieces criticising the Church of England for welcoming and caring for transgender children. Sadly many of these opinion pieces are deeply misinformed of the facts.
There is much misinformation on the subject of transgender children and everyone has a view – I’m reminded of ‘Send us your reckons’ from Mitchell and Webb.
Sadly this misinformation has led to very real consequences for families with transgender children. We know Christian grandparents who have stopped all contact with transgender grandchildren. We know vulnerable families with transgender children who do not feel welcome in their place of worship.
Positive examples of church acceptance, kindness and inclusion (and thankfully in the UK there are many more good stories than bad) are included at the end of this post.
Any Christians commentating in this area, particularly those with a platform and a following, have a moral responsibility to make themselves familiar with the facts, not simply regurgitate the propaganda of anti-transgender lobby groups, (unless they are part of those groups which seek to restrict the rights of LGBT youth).
I’ve taken as an example a recent article by Ian Paul, expressing deep concern about a move towards “unthinking and unqualified affirmation of those asking for recognition of their transgender status, even if motivated by kindness”. I chose to focus on this article as Ian apparently is open to learning and hearing additional information on this subject. I am happy to share in good faith information with anyone open minded enough to listen. Here therefore is a detailed response to his post (quoted at length in the blue boxes):
“then what of the far more complex question of gender identity?
The famous obstetrician Robert Winston was drawn into the controversy around this question on Radio 4 last week. He pointed out the serious harm that can arise from medical intervention to effect gender ‘transition’.
Speaking on the Today Programme on BBC Radio 4, he said that “results are horrendous in such a big proportion of cases”. He said 40 per cent of people who undergo vaginal reconstruction surgery experience complications as a result, and many need further surgery, and 23 per cent of people who have their breasts removed “feel uncomfortable with what they’ve done”.
He added: “What I’ve been seeing in a fertility clinic are the long-term results of often very unhappy people who now feel quite badly damaged. One has to consider when you’re doing any kind of medicine where you’re trying to do good not harm, and looking at the long-term effects of what you might be doing, and for me that is really a very important warning sign.”
The ‘famous obstetrician’. You are quoting the views of someone who has no experience in treating, much less in performing surgery on, transgender people. The statistics he provides do not accord with the evidence based views of specialists who are clear that transgender surgery has one of the best outcomes of all types of surgery:
This is from those with real expertise treating transgender people, the Endocrine Society:
“Medical intervention for transgender individuals (including both hormone therapy and medically indicated surgery) is effective, relatively safe (when appropriately monitored), and has been established as the standard of care.”
Winston refers to two references which do not appear to support his assertions:
Complications of the Neovagina in Male-To-Female Transgender Surgery: A Systematic Review and Meta-Analysis With Discussion of Management PC Dreher et al. Clin Anat. 2017 Oct 23
Postoperative Complications Following Primary Penile Inversion Vaginoplasty Among 330 Male-To-Female Transgender Patients TW Gaither et al. J Urol. 2017 Oct 11
Here are two quotes from the first paper:
“Wagner et al. (2010) describe that gender reassignment surgery (GRS) has proven to be the best solution for patients with discordant gender and contributes significantly to psychosocial stability in these patients”
“An increasing number of patients appear to be seeking this surgery, likely due in part to increasing acceptance by medical and reimbursement communities, high satisfaction rates and improved quality-of-life reports according to Gooren (2011).”
This first paper (Dreher et al) covers surgery worldwide since 1995 and produces an average of 21% of patients requiring additional procedures. It notes that rates of complication are very significantly lower (nearing 0%) in surgeons who have conducted more than 40 surgeries. This suggests improved surgical guidance and training is key to improved outcomes.
The second paper (Wagner et al) looks at the work of an experienced surgeon, and notes 9% required a follow on procedure, almost all of these were conducted as an outpatient and none were severe complications (none graded IV or V). It concludes it is a relatively safe procedure.
It should be recognised that talking about surgery in relation to children is a common tactic used by transphobic groups to misinform and provoke fear. No children in the UK NHS have surgical interventions (the minimum age for surgery is 18).
“For expressing his informed medical opinion, Winston received a torrent of hate mail from transgender activists.”
There is a climate of fear mongering and misinformation in the media about transgender people and transgender children, fuelled by lobbyists such as Christian Concern. I do not condone any hate mail. I do however, understand people expressing their deep frustration at a respected professor using their voice to spout misinformation on a public platform.
Winston’s Daily Mail article follow up is titled “Trolls call me homophobic” which suggests some really basic misunderstanding of the difference between homophobia and transphobia.
You could read this humorous blog post which provided some light relief for those of us who have seen this all before.
Although I describe myself as transgender (I was donning flamboyant male costumes from early childhood on),”
Camille here is describing gender expression (what clothing they like) rather than gender identity (who they are). Clothing does not make a person transgender. This is someone who has a history of appropriating a transgender identity as a rhetorical device with the goal of curtailing the rights of transgender people.
Along with Prof Winston, Camille Paglia also has no known expertise in supporting transgender people
“I am highly sceptical about the current transgender wave, which I think has been produced by far more complicated psychological and sociological factors than current gender discourse allows.”
The phrase ‘transgender wave’ is distorted and dehumanising language. The increase in people seeking support means less people are struggling on their own. Here are the words of experts from the Australian Standards of Care and Treatment:
“with increasing visibility and social acceptance of gender diversity in Australia, more children and adolescents are presenting [….and ] requesting support, advice, and gender affirmative psychological and medical treatment”. They note that with “approximately 1.2% of adolescents identifying as trans […] it is likely that referrals will continue to rise in the future”.
See this thread on twitter which makes a comparison between the current increase in numbers of out transgender people (and referrals to youth gender services) with the rise in prevalence of left handed people last century: https://twitter.com/DadTrans/status/929081990107881472
(In short – in 1900 there was significant social prejudice against left handed people – left handed children were forced to write with their right hand – and only 2% of the population was openly left handed. With increased acceptance of left-handed children, numbers of openly left-handed people rose sharply in the early twentieth century and have remained constant at about 12% of the population since then. Speculators in the 1930s could have expressed concern about the sharp increase in left-handedness. But the phenomenon was clearly related to increasing levels of acceptance leading to left-handed people being more open and not having to pretend to be right-handed. Interestingly, in Japan where there is still stigma and left-handed children are still forced to use their left hand, the prevalence is still 2%).
“Furthermore, I condemn the escalating prescription of puberty blockers (whose long-term effects are unknown) for children. I regard this practice as a criminal violation of human rights.”
This is the ideologically based opinion of someone with no qualifications in this topic. Puberty blockers are safe and reversible. They have been prescribed for precocious puberty since the 1970’s and continue to be prescribed for this purpose (delaying the puberty of children who begin puberty too young).
“Puberty delaying hormones …have the following benefits: a. The main benefit of early physical treatment is arrest of pubertal development, and, consequently, arrest of the suffering of the patient (CohenKettenis et al., 2003, p. 171). b. Arresting the progress of puberty gives adolescents more time in which to achieve greater certainty about their innate gender identity. c. The administration of blockers will prevent the development of secondary sexual characteristics of the undesired sex. In turn, future treatment would be less invasive and painful (for example, breast removal in female-to-male patients and painful and expensive treatment for facial hair in male-to female patients will be prevented; the voice will not deepen, and nose jaw and crico-cartilage (Adam’s apple) will be less developed)) (Cohen-Kettenis et al., 2003, p. 171). d. Successful adaptation is associated with early start of physical treatment (Cohen-Kettenis et al., 2003, p. 171)”.
The safety and reversibility of puberty blockers are looked at in the recent Australian national medical guidance (published September 2017) which states:
“Puberty suppression is most effective in preventing the development of secondary sexual characteristics when commenced at Tanner stage 2”. ”reduction in the duration of use of puberty suppression by earlier commencement of stage 2 treatment must be considered in adolescents with reduced bone density to minimise negative effects.”
“We suggest that adolescents who meet diagnostic criteria for GD/gender incongruence, fulfil criteria for treatment, and are requesting treatment should initially undergo treatment to suppress pubertal development
These recommendations place a high value on avoiding an unsatisfactory physical outcome when secondary sex characteristics have become manifest and irreversible, a higher value on psychological well-being, and a lower value on avoiding potential harm from early pubertal suppression.”
Start puberty before blockers
“We suggest that clinicians begin pubertal hormone suppression after girls and boys first exhibit physical changes of puberty.
We recommend treating gender-dysphoric/gender-incongruent adolescents who have entered puberty at Tanner Stage G2/B2 by suppression with gonadotropin-releasing hormone agonists.”
Here’s the criteria for blockers, which are not handed out on a whim:
Criteria for blockers
“Adolescents are eligible for GnRH agonist treatment if:
A qualified MHP has confirmed that:
the adolescent has demonstrated a long-lasting and intense pattern of gender nonconformity or gender dysphoria (whether suppressed or expressed),
gender dysphoria worsened with the onset of puberty,
any coexisting psychological, medical, or social problems that could interfere with treatment (e.g., that may compromise treatment adherence) have been addressed, such that the adolescent’s situation and functioning are stable enough to start treatment,
the adolescent has sufficient mental capacity to give informed consent to this (reversible) treatment,
And the adolescent:
has been informed of the effects and side effects of treatment (including potential loss of fertility if the individual subsequently continues with sex hormone treatment) and options to preserve fertility,
has given informed consent and (particularly when the adolescent has not reached the age of legal medical consent, depending on applicable legislation) the parents or other caretakers or guardians have consented to the treatment and are involved in supporting the adolescent throughout the treatment process,
And a paediatric endocrinologist or other clinician experienced in pubertal assessment
agrees with the indication for GnRH agonist treatment,
has confirmed that puberty has started in the adolescent (Tanner stage $G2/B2),
has confirmed that there are no medical contraindications to GnRH agonist treatment.”
“The cold biological truth is that sex changes are impossible. Every single cell of the human body remains coded with one’s birth gender for life. Intersex ambiguities can occur, but they are developmental anomalies that represent a tiny proportion of all human births.”
Does this author actually believe that transgender people do not exist? This is a deeply transphobic perspective and the fact that the author describes herself as transgender does not undo the clear transphobia here. Camille also clearly does not understand the difference between sex and gender.
Intersex ambiguities are estimated by WHO to be 1% of births which is hardly a tiny proportion.
Futhermore, the findings of the Endocrine Society note conclusive evidence of ‘a biological underpinning for gender identity’ and list the many scientific studies noting a biological underpinning. Below I’ve provided the cold biological truth about transgender people as written by the global experts in endocrinology
In September 2017 the Endocrine Society published a guideline, entitled “Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline,” (published online and will appear in the November 2017 print issue of the Journal of Clinical Endocrinology & Metabolism (JCEM), a publication of the Endocrine Society). This updated guidance was produced by leading endocrinologists specialising in support to transgender adults and adolescents from the US, Belgium, and the Netherlands. The guidelines are endorsed by the American Association of Clinical Endocrinologists, the American Society of Andrology, the European Society for Pediatric Endocrinology, the European Society of Endocrinology, the Pediatric Endocrine Society, and the World Professional Association for Transgender Health.
“The medical consensus in the late 20th century was that transgender and gender incongruent individuals suffered a mental health disorder termed “gender identity disorder.” Gender identity was considered malleable and subject to external influences. Today, however, this attitude is no longer considered valid. Considerable scientific evidence has emerged demonstrating a durable biological element underlying gender identity. Individuals may make choices due to other factors in their lives, but there do not seem to be external forces that genuinely cause individuals to change gender identity.
Although the specific mechanisms guiding the biological underpinnings of gender identity are not entirely understood, there is evolving consensus that being transgender is not a mental health disorder. Such evidence stems from scientific studies suggesting that: 1) attempts to change gender identity in intersex patients to match external genitalia or chromosomes are typically unsuccessful; 2) identical twins (who share the exact same genetic background) are more likely to both experience transgender identity as compared to fraternal (non-identical) twins; 3) among individuals with female chromosomes (XX), rates of male gender identity are higher for those exposed to higher levels of androgens in utero relative to those without such exposure, and male (XY)-chromosome individuals with complete androgen insensitivity syndrome typically have female gender identity6; and 4) there are associations of certain brain scan or staining patterns with gender identity rather than external genitalia or chromosomes
In summary, although there is much that is still unknown with respect to gender identity and its expression, compelling studies support the concept that biologic factors, in addition to environmental factors, contribute to this fundamental aspect of human development.”
“Data are strong for a biological underpinning to gender identity”
“All of this”. All of what? You have quoted two people with no expertise or experience.
A clearer interpretation is that the General Synod has moved towards being compassionate to transgender people, in line with recent scientific research and expert endorsed best practice.
“Winston is pointing out the (unintended) consequences of hasty and naive action in this area, just as Jon Kuhrt is pointing out the results of hasty and naive action in response to the homeless. There are the consequences of giving an unthinking and unqualified affirmation of those asking for recognition of their transgender status, even if motived by kindness. It is, in any complex situation, quite possible to harm even when intending to do good, if care and love are not shaped by awareness and wisdom. What is true of those asking for money is true of those asking for recognition. These are the facts that the Church needs to take account of; in fact, these are the things any of us needs to take account of if we are to be wise and compassionate pastors.”
To be wise and compassionate pastors you should follow the guidance provided by those who are best qualified in this topic. The actual experts. Transgender people exist. Transgender people have always existed. There is a “durable biological underpinning to gender identity” (Endocrine society).
Here’s several quotes from Australia’s Standards of Care:
“being trans or gender diverse is now largely viewed as being part of the natural spectrum of human diversity”.
“increasing evidence demonstrates that with supportive, gender affirmative care during childhood and adolescence, harms can be ameliorated and mental health and well being outcomes can be significantly improved”.
“Avoid causing harm”. “withholding of gender affirming treatment is not considered a neutral option, and may exacerbate distress in a number of ways including depression, anxiety and suicidality, social withdrawal, as well as possibly increasing chances of young people illegally accessing medications”
“for children, family support is associated with more optimal mental health outcomes”
“trans or gender diverse children with good health and wellbeing who are supported and affirmed by their family, community and educational environments may not require any additional psychological support beyond occasional and intermittent contact with relevant professionals in the child’s life such as the family’s general practitioner or school support”.
Australia’s Royal Children’s Hospital Gender Service new “Australian Standards of Care and Treatment Guidelines for Trans and Gender Diverse Children and Adolescents”. These guidelines are compiled by the leading Australian experts, based on the best and most current evidence from around the world. These guidelines are endorsed by ANZPATH (the Australian and New Zealand Professional Association for Transgender Health) and were launched at the recent ANZPATH conference. They are now the official guidelines for all health professionals working with transgender children in Australia.
“Transgender trend” are a non-religious group representing parents of children with gender dysphoria who do not agree with the current transgender ideology. They made a presentation to the Government, opposing the planned demedicalisation of the legal process around ‘transition’. I reproduce below some of the facts they set out—facts that the Church of England will need to take into account in anything that it proposes in this area as part of its wider debate on sexuality.”
“Transgender trend” are considered by parents of transgender children like myself as an anti-transgender hate group. Their posts, publications and tweets are deliberately incendiary, malicious and frequently based on an extremely biased review of evidence. They pose as ‘concerned parents’ but constantly attack the rights of transgender people in general and transgender children in particular. Their website is neither neutral, nor concerned for the well-being of transgender children. The key individuals on the site do not have transgender children. The group name “transgender trend” should give you a clue. These are not experts but a small group with the sole agenda of undermining the well being of transgender children. Why not quote from the highly respected charity Mermaids, who has over 1,000 parent members, all parents of transgender children in the UK. Mermaids co-hosted with the NHS the 2017 conference on trans children that you quote in one of your sources. “Transgender trend” meanwhile is a fringe anti-trans lobby group without credibility.
“I also speak to urge caution on behalf of the children of this generation who are caught up in the teaching of a new rigid, anti-science belief system presented to them as fact.”
The Endocrine Society are scientists. Supporting transgender children is evidence based science. Please provide a source that supporting transgender children is anti-science
“If Gender Identity is established in law as a Protected Characteristic, it will apply to children of any age. But a child’s identity is not fixed: it changes over time, and it is shaped by factors like parental approval and societal influences. If all trusted adults are reinforcing daily a little boy’s belief that he is really a girl, this will have an obvious self-fulfilling effect. Puberty blockers supply the ‘answer’ to the created fear of a puberty he now believes to be the ‘wrong’ one.”
You are quoting a transphobic view here that is completely inaccurate. Let me explain:
A) You are suggesting that parents are imposing or reinforcing a child’s gender identity. The Lancet report is clear:
“research has established no clear correlations between parenting and gender incongruence”
B) You are suggesting that parental denial of a child’s identity will make them less likely to be trans
Here’s the Endocrine Society:
“The medical consensus in the late 20th century was that transgender and gender incongruent individuals suffered a mental health disorder termed “gender identity disorder.” Gender identity was considered malleable and subject to external influences. Today, however, this attitude is no longer considered valid. Considerable scientific evidence has emerged demonstrating a durable biological element underlying gender identity.1,2 Individuals may make choices due to other factors in their lives, but there do not seem to be external forces that genuinely cause individuals to change gender identity.”
3) You are claiming that a trans girl is a boy who is deluded and wrong.
The Endocrine Society concludes:
“a durable biological underpinning to gender identity”
The World Professional Association of Transgender Health and ICD are removing the classification as a mental health disorder, acknowledging that it is natural human variation. Note these bodies are slow moving – ICD only de-classified homosexuality as a mental disorder in 1992
“While researchers have much to learn about gender-expansive and transgender children, there is evidence that both reparative therapy and delayed transition can have serious negative consequences for children. While some groups promote these strategies in good faith, many use misleading descriptions of research or even outright misinformation.”
“Almost all children on blockers progress to cross-sex hormones at age 16. [2] Very few come off this path of increasingly invasive medical treatments once they are on it and so-called ‘social transition’ is the first step. This approach clearly works to prevent normal resolution of childhood gender dysphoria and foster persistence of opposite-sex identity.”
The protocols for receiving blockers in the NHS are exceedingly conservative. Families first need to get a referral from a GP, which many GPs are unwilling to provide. Many are sent on a time-consuming detour via the child mental health service CAHMS (until CAHMS confirm gender identity is not a mental health issue and refer on to the Gender Identity service). Once referred to the Gender Identity Service there is a 12 month wait for first appointment. Then a 6 month assessment process. Then prolonged monthly sessions with psychologists talking about identity. Even then blockers are very far from guaranteed – a young person can only get blockers if referred from the NHS Gender Service, and they are extremely conservative. Only the most persistent children, the ones with the most clear cut and long held identity, the ones who insist session after session and show no doubt, who are supported by their parents, who are usually socially transitioned and accepted as their identified gender in their lives – these are the very small number of children who are referred for blockers. It is not surprising to me that the small number of children who jump through all the medicalised hoops for years and years to get blockers, are likely to continue in their identity.
“Certainly the studies listed in the 2016 paper provide no conclusive evidence that consistent, persistent, insistent transgender children are likely to desist. In fact the best of these bad studies does not support desistance at all, but instead clearly showed a 58% persistence rate”.
To talk about it as a ‘path’ is also extremely misleading. Whilst many transgender adolescents (none before the age of 15 years 10 months on the NHS) end up eventually taking hormones, not all will have further interventions such as surgery (and surgery is never available in the NHS before age 18).
“While trans activists call for the de-medicalisation of ‘transgender,’ in the case of children they campaign aggressively for social transition, blockers and cross-sex hormones at ever earlier ages”
Again, this is couched in unnecessarily incendiary language such as “at ever earlier ages”. Advocates for the rights of transgender children understand that puberty blockers should be prescribed at the start of puberty (otherwise they have no purpose – there really is a clue in the name). Concerned parents are conflicted about the advice on the ideal age for cross-sex hormones, with some experts arguing for this to start at around age 16 (as is the current NHS protocol even though for many children it is late in their pubertal developmental) whereas some experts are arguing for the prescription at a younger age. This debate on appropriate age for cross-sex hormones is ongoing and is outlined in the Endocrine Society’s guidance and it is right that this .This debate is not one between transgender activists and concerned parents, it is a debate between competent medical professionals who are currently divided and who take different value judgements when deriving their approach. Your blog post could have presented this in an informed and sensitive way – instead of repeating the material espoused by the group called “transgender trend” who do not believe in the existence of transgender children.
“The surge in sex hormones at puberty triggers the enormous changes in the teenage brain which don’t complete their job until the mid-twenties. [4] The brain /personality is not fully-formed until then. The effects of blockers on adolescent brain development are unknown [5] although studies on adults, including men taking the drug for prostate cancer, indicate risk of memory loss, depression and cognitive impairment. [6] Recent reports from the US indicate long-term serious health effects for women who were administered blockers for precocious puberty, such as excruciating muscle and bone pain, depression, weakness and fatigue.”
The potential dangers of puberty blockers need to be weighed up against the very real and known impacts of a transgender person going through the wrong puberty. People who recognise the existence of transgender people are very aware of this balance. “Transgender trend” does not acknowledge (or care) about transgender people so only presents potential negatives.
Here’s the take from the Australian specialists in their guidance published this year:
“Avoid causing harm”. “withholding of gender affirming treatment is not considered a neutral option, and may exacerbate distress in a number of ways including depression, anxiety and suicidality, social withdrawal, as well as possibly increasing chances of young people illegally accessing medications”
“Preventing a child’s sexual development in early puberty, followed at 16 by cross-sex hormones, results in sterility as viable eggs or sperm have not developed”
It is accepted that cross-sex hormones can be a barrier to fertility in many youth, though this is not a reason to withhold necessary treatment. This is a discussion to be had, but it needs to be held much more sensitively based on an understanding of the needs of transgender adolescents and adults. For any individual and any family, difficult discussions around fertility are core to any decision about cross-sex hormones – this is not rushed in to on a whim, and counselling about potential impact on fertility is a requirement before eligibility.
“These children are prevented from ever experiencing puberty: hormones can only superficially feminise or masculinise secondary sex characteristics, they cannot create the puberty of the opposite sex”
This is a non-scientific statement that shows very limited knowledge of endocrinology.
“Risks of cross-sex hormones include cardiac disease, high blood pressure, blood clots, strokes, diabetes and cancers. [9] Some significant effects are irreversible, such as male-pattern baldness and body and facial hair, masculinised voice and compromised fertility.”
All medical treatments have potential side-effects. If I listed the potential side effects of paracetamol without context it would look similarly alarming. This is intentionally inflammatory.
“There have been no clinical research trials into the long-term effects of this treatment on children”
We have over 20 years of data with no ill effects observed in that period. We’d of course like more data and this will come in time. We do conversely have plenty of long term evidence of the poor outcomes (particularly in terms of mental health, depression, wellbeing) for transgender adults who have not been supported and accepted in childhood. Concerned parents are hoping for a better outcome for their own children, and the latest evidence, including from the Netherlands, is very positive.
“this is a non evidence-based practice [10] to treat a non evidence-based diagnosis of being ‘a girl trapped in a boy’s body’ and vice versa [11] and this generation of children are the guinea pigs.”
This is a ‘Straw man argument’. There is no diagnosis of ‘being a girl trapped in a boy’s body’. This is a phrase that some transgender people in the past have used to try to explain in simple terms how they feel. This is not a scientific diagnosis and no one claims this is the situation. What is known is that some children have a clear and consistent gender identity that differs from the sex they were assigned at birth. Experts have found “conclusive evidence that there is a durable biological underpinning for gender identity” – speculated to be due to hormone fluctuations in utero.
As a concerned parent I would much rather be living 40 years in the future when there is better long term data. However, this is not in itself reason for with holding treatment. We have to make the best evidence based decisions we can based on what is currently known. Again here’s a quote from the Australian national health guidelines:
“withholding of gender affirming treatment is not considered a neutral option, and may exacerbate distress in a number of ways including depression, anxiety and suicidality, social withdrawal, as well as possibly increasing chances of young people illegally accessing medications”.
“‘Transgender’ is an ideological label distinct from the clinical diagnosis ‘gender dysphoria.’ To call a child ‘transgender’ is to make both a claim that the child’s feelings represent material reality and a prediction about that child’s future: they will not change.”
Unlike the apparent anti transgender ideology of the author quoted, transgender is not an ideology. Transgender is an adjective to describe people whose gender identity is different to the sex they were assigned at birth from a cursory inspection of their genitals.
“An analysis of all published research studies of children with ‘gender dysphoria’ shows that 80% will naturally come to be happy as the sex they were born and this is true of even some of the most severe cases, we can’t know which children will persist and which will desist.
Opposite-sex identity in childhood is overwhelmingly predictive of gay or lesbian sexual orientation in adulthood, not transsexualism.”
This statement is demonstrably false and shows the people at “Transgender Trend” are intentionally conflating the distinction between children who are gender non-conforming (eg boys who like dolls) and children who are transgender (eg children assigned male at birth who have a consistent, insistent and persistent identity that they are a girl). The research that gave rise to the myth of 80% ‘desistance’ has been comprehensively discredited as deeply flawed and unreliable as it lumped together gender non-conforming and transgender children – In fact:
“Certainly the studies listed in the 2016 paper provide no conclusive evidence that consistent, persistent, insistent transgender children are likely to desist. In fact the best of these bad studies does not support desistance at all, but instead clearly showed a 58% persistence rate).
“Affirming a child’s ‘gender identity’ can therefore be seen as gay conversion therapy by another name.”
Gender identity and sexual orientation are two separate things. Some transgender people are homosexual, some are heterosexual, some are bisexual, some are pansexual (attracted to people regardless of gender including non-binary people). The same therapists who attempted ineffectual and harmful conversions of gay people later applied the same techniques to attempt conversion of transgender children.
“There has been an almost 1000% increase in children referred to the Tavistock clinic in London over the past 6 years. [14] These figures are inflated by the unprecedented rise in the number of girls – nearly 70% of the figure overall and over 70% of adolescent referrals last year. [15] By comparison, in the late Sixties 90% of adult transsexuals were male. [16] We are aware that teenagers and young adults are susceptible to indoctrination, brainwashing and social contagion which is why we block online anorexia and self-harm sites. The internet, however, is chock-full of Tumblr bloggers and Youtube vloggers with hundreds of thousands of followers, who are selling vulnerable young people the myth of transformation through cosmetic alteration of their bodies, including amputation of healthy body parts, and a lifetime’s dependency on powerful off label hormones.”
I’ve mentioned prevalence earlier in this response (see above). This increase in numbers referred to the UK Gender Identity Service (GIDS) was not unexpected or unusual but predicted, as was the increase in assigned female referrals (specialists had predicted years ago an increase in assigned female referrals). Yes, it is a fact that there are a few openly trans people on the internet – individuals who are followed by individuals who before the availability of the internet would have been completely on their own. Isn’t it wonderful that now a few trans people are sharing their experiences, offering support to isolated transgender people. The remainder of the quoted section is pure conjecture and hyperbole.
“Recent reports of girls’ mental health indicate that girls and young women in the UK are in crisis. [17] Recently published evidence of the rate of sexual abuse and harassment in schools across the UK is a matter of national shame. [18]
Reports such as the recent Stonewall Schools Report [19] which indicate high suicidal ideation in ‘trans’ youth serve to cover up the fact that the vast majority of these youngsters will be teenage girls, now hidden in the category ‘trans boys.’”
The Stonewall report indeed outlines what a tough time transgender children are having at school. Media hysteria, continual criticism, and trans boys being described as girls is exactly what makes life hard for a trans child or adolescent. The C of E guidance supports acceptance of all people, even those who are different. It encourages schools to be welcoming safe places where transgender children can get an education without harassment or bullying. Who would want more bullying of transgender children? The C of E guidance is extremely sensible and should be welcomed by all who care about children. In the past schools were not welcoming places for children who were different. This did not mean these children didn’t exist– it just left them bullied, depressed, ashamed and needing to hide.
“A PSHE teacher and Head of Year at a large comprehensive told me that in her school the kids who identify as ‘trans’ are, without exception, either lesbian, autism spectrum, have mental health problems or have suffered sexual abuse.”
This kind of rhetorical anecdote is a well worn device familiar to anyone who has watched a political debate. For an easy to digest discussion on this phenomenon see http://www.bbc.co.uk/news/uk-politics-20956126
Sexuality and gender identity are different concepts, something this teacher seems confused about.
Many trans children suffer mental health problems such as depression – this is recognised as ‘minority stress’. Depression, stress and anxiety not because of who they are but because of how they are treated.
Supporting trans children is the best option for those who genuinely care about their wellbeing. I’m glad the Church of England has been informed by experts and those who know trans children.
“Parents are also concerned about the relentless gender identity propaganda their children are subject to today – across the media, [20] the internet and in schools, through organisations such as GIRES, Gendered Intelligence, Mermaids and Educate and Celebrate. The belief that gender is an innate identity is taught to children as truth, with no alternative views offered, in contravention of the UN Rights of the Child.”
Trans children exist. They have always existed. And the few quiet voices speaking up for them are dwarfed by the powerful anti-trans voices that are platformed daily across tv, newspapers and radio. As I write this, in the last week, The Times alone has published 7 articles attacking trans children. The reality is that anti transgender rhetoric is prominent and inescapable, much to the distress of transgender children, adults and their friends and families.
“The ‘transition or suicide’ trope is repeated endlessly, against all Samaritans guidelines. There is no evidence that children will commit suicide if their parents fail to support them in taking a medical pathway, but of course the threat terrifies parents into feeling they have to.”
I agree that writing about suicide needs to be handled sensitively and in accordance with the Samaritans guidance. Seeing as you raised this, (as anecdote, and without irony, in the same sentence as saying it shouldn’t be mentioned), here’s a statement of evidence from the Endocrine Society:
“Transgender individuals who have been denied care show an increased likelihood of committing suicide and self-harm”
“There are over 260 trans youth support groups across the UK [21], which provide the ‘tribe’ where our most vulnerable young people will be accepted, maybe for the first time, as long as they identify as trans. All transgender organisations advertise their support for ‘gender non-conforming’ youth, sweeping up all children who are ‘different’ and don’t fit in.
These organisations claim to support ‘diversity’ but of course they do the opposite: a girl who rejects feminine stereotypes is transformed into a ‘boy’ who conforms to masculine stereotypes. Gender non-conformity is erased. Regressive and reactionary sex-stereotyping is being sold to young people as a progressive social justice movement.”
This shows very little knowledge of these organisations and their scope. A girl who rejects feminine stereotypes would not be ‘transformed’ by a youth group into a boy who conforms. My transgender daughter is not a cliché or a stereotype of femininity. She likes football and art, wears jeans more than dresses, and is a normal well rounded child with a variety of interests and likes. The majority of transgender children and adults I know are defiantly breaking down gender stereotypes. It is “Transgender Trend”, who seem set on reducing trans children to the regressive stereotypes they claim to be against. At this point I doubt very much whether they have even met any transgender children.
“To teach children that their ‘authentic self’ is something in their heads, split off from and in opposition to, the body, is to create gender dysphoria. Mind-body disassociation is recognised as a state of mental ill-health: in this case uniquely, it is presented as a normal variation and something to be celebrated. Mental health is based on being equipped to accept reality.
Since children have been taught that it is their ‘gender identity’ which makes them a boy or a girl and not their biological sex, calls to Childline from young people confused about their gender have doubled in a year – eight calls are now received every day from children as young as eleven. [22] The concept of ‘gender identity’ is clearly – and inevitably – causing mental health problems for young people.”
Again the author deliberately and falsely presents transgender people as mentally ill, deluded or confused. Throughout the 20th century, methods were applied to trans people to stop them being trans including electroshock and attempted conversion therapies. These techniques, historically used also on gay people, disabled people, and other marginalised groups, did not work. Instead trans people were harmed with resulting depression and shame. All forms of conversion therapy are now seen as both unethical and ineffective.
“Any child who suffers genuine gender dysphoria must of course be sensitively supported in schools and youth organisations. But teachers, professionals and other children cannot be asked to collude in the reinforcement of a child’s belief which contradicts reality. Recognition of biological facts is not bigotry.
When girls are told that a male classmate is now a girl, their sense of their own reality is shattered. If a biological male is a girl, then it is not female biology which makes you a girl, it is something else. Girls must look to a male classmate to find out the invisible magic quality they need, and the boy is given the power to define what a girl is. We cannot predict the long-term practical or psychological effects on girls taught to deny their own biology, without the right to even define themselves correctly as the female sex.”
This is denial that trans people exist. This is extremely disturbing and appears to be advocating for teachers not to work in accordance with the 2010 Equality Act. This damaging bigotry harms children like mine who just want to live their life without prejudice. This also shows no understanding of the complexities of biology.
“If teenage girls must consent to a male classmate using their toilets and changing-rooms they learn that their boundaries may be violated and their consent is unimportant. Girls learn that they are not always allowed to say ‘no.’ This is grooming; lessons on the importance of consent become meaningless.
Girls who are coached at school into ignoring their own discomfort and intuition may go on to put themselves in risky situations with any man who claims to be a woman, out of fear of being seen as transphobic.
In the case of public swimming pool changing rooms a young girl cannot name a male with a penis as a man: voyeurism and indecent exposure cease to exist as crimes if a man claims to be a woman. Normal child protection protocols effectively become unlawful.”
This rhetoric is now moving beyond bigotry towards hate. It reveals what was clear from the start, there is no care for transgender children, but simply hate rooted in fear. These exact same arguments were put forward against gay people in the 1980s and gave rise to Section 28.
I am deeply concerned that we are not learning from the lessons of the past, and that history may repeat itself, with transgender people the latest in a long history of marginalised groups being attacked, stigmatised and othered.
Trans women are women. Trans girls like my daughter are girls. They are not a threat.
For anyone wanting to sensitively address the stance of organised religion to trans issues then the following must be the foundation for any discussion: Trans people exist; Trans people have always existed; Trans children exist.
If you choose to comment on these issues, you can do as this writer has done whether maliciously or through ignorance, and seek to marginalise trans people, present them as mentally deluded or potentially dangerous, encourage others to fear and reject them.
Or, instead, you can choose to embrace them, tell them you love and accept them as they are. My own grandparents were deeply committed Christians and I know they would have loved and supported my daughter. Please open your eyes and your hearts. Tell transgender children and their families that they are welcome in your schools and even in your churches (temples, mosques etc). Commit to protecting vulnerable transgender children from bullies including uniformed writers who spread misinformation, hate and fear.
To the Church of England. I am grateful that The Church of England have bravely ignored media hysteria and stood up for one of the most misunderstood, marginalised and attacked groups of children.
I commend them for caring for my transgender child.
To conclude here (with permission) are positive stories of Church and Christian community acceptance, inclusion and love:
“Our C of E/Methodist church has been very supportive. We often have talks on inclusivity and the love of God. My daughter also goes to a C of E school and the message we’ve had there is one of acceptance and kindness. In fact the head teacher said that as a Christian school they should be the first to show kindness and acceptance, and zero tolerance to any kind of unkindness.”
“We’re so lucky, our C of E church have been wonderful”
“We were at our previous church when our child socially transitioned. My husband was suddenly asked to stop doing sermons in church. We ended up going to another church. Our new church however have been incredible, from day one they used our child’s pronouns, and when he chose a new name a month after we joined the church absolutely everyone began using it immediately. They’ve been nothing but supportive and accepting.”
“The vicar at our c of e place was just calmly accepting and kind when I told her about my child. It’s a Church that does loads of social justice stuff and has a welcoming, un-judgemental attitude in general.”
“A Sunday School teacher was the first one to tell me that my child was using a different name. We attend the Church of Scotland. If you look at who Jesus was actually hanging out with it’s fairly clear to me that Christians are called to support people who are perhaps a little bit different and not accepted by wider society.”
“So far I have been surprised by our religious relatives (Jehova’s Witnesses and Christians), I was expecting some discomfort from them but they have all been supportive and accepting.”
“The poignant words of my eldest daughter’s blog detailing our family’s sad estrangement from the local CofE church. https://bethmackin.wordpress.com/…/may-2017-faithfully…/ We left said church and now attend a inclusive church that is a URC/Methodist church. I feel much safer, loved and cared for but mourn the loss.”
“Many positive examples to be found at Diverse Church – a UK wide organisation with groups for 18-30 LGBTA+, they also have a parents forum that has a specific hub for Christian Parents of Transgender children http://diversechurch.website/
See also OneBodyOneFaith – Great for engagement with current issues as well as networking to find safe and accepting churches. http://www.onebodyonefaith.org.uk/ and OpenTable which is a collection of LGBT inclusive eucharist services. This Sunday Open Table London will hold a special service for Transgender Day of Remembrance https://www.facebook.com/opentablelondon/”