New Zealand has produced guidance for trans healthcare: Guidelines for gender affirming healthcare for gender diverse and transgender children, young people and adults in Aotearoa New Zealand
This follows similar guidelines produced in the US (by the world’s largest paediatric medical organisation the American Academy of Pediatics), Australian affirmative healthcare guidance for transgender children and adolescents, and similar practices in place for trans children and adolescents across Canada, Spain, Germany
New Zealand’s gender affirmative healthcare guidelines for transgender children, yet again shows the UK GIDS is stuck in the dark ages, the UK NHS is failing transgender children.
Here’s a ten point summary (written by me) for those disinclined to read further:
- New Zealand endorses gender affirmative healthcare for trans children and adolescents.
- New Zealand acknowledges that some children are trans at a young age, that some adolescents come to understand their gender identity at or after puberty, and that all are valid and in need of affirmation and support.
- New Zealand uses modern, trans positive language and does not problematise trans children, being clear that trans children who are supported should be able to thrive and should be able to be as happy as any other child.
- New Zealand supports social transition for trans children, emphasising the important benefits and protective aspects for their well-being.
- New Zealand recognises the importance of supportive families, and prioritises educating parents/carers to accept and affirm their trans children, providing clear and reassuring guidance to listen to their child.
- New Zealand is clear that gender affirmative healthcare is medically necessary, considering a range of aspects of health including support in dealing with minority stress.
- New Zealand supports access puberty blockers, which it emphasises are reversible. It emphasises that withholding timely access to blockers causes harm, and emphasises that not using blockers can lead to irreversible unwanted physical changes.
- New Zealand supports individualised access to hormone therapy, acknowledging the compelling reasons why access prior to age 16 is appropriate for some individuals. It provides clear information on the changes that are reversible, partially reversible, not reversible and the time on HRT for these changes to emerge.
- New Zealand acknowledges the harm caused by the pathologisation of gender diversity, and commits to depathologisation within the health service. New Zealand acknowledges being gender diverse is not a mental health condition and commits to mental health support being optional and not a mandatory part of accessing affirmative healthcare.
- New Zealand acknowledges the negative health impacts of discrimination, and acknowledges the importance of health service providers advocating for trans people, advocating for social and public policy change to reduce the negative effects of minority stress.
This blog summarises the main areas of the New Zealand guidance that are relevant for trans children and adolescents, highlighting areas where New Zealand’s healthcare guidance for trans children is ahead of the UK NHS (I use the word ahead rather than different, as there is a clear trajectory for trans children’s healthcare globally – I have no doubt the UK will eventually make a change in this direction – as have already done Australia, much of USA and Canada, Spain, Germany etc – It just remains to be seen how many years the UK will cling on to outdated practices, and how many children will be harmed in the meantime.
The New Zealand Guidelines: An Overview
*Note: The guide is written with many references to Maori terms and indigenous approaches. This heavily abridged version aimed at a UK and global readership just includes English terms – the guidance is worth reading in full.
Commits to gender affirming healthcare (UK GIDS does not offer this)
“Gender affirming healthcare (definition): “Healthcare that is respectful and affirming of a person’s unique sense of gender and provides support to identify and facilitate gender healthcare goals. These goals may include supporting exploration of gender expression, support around social transition, hormone and/or surgical interventions. This may also involve providing support to family, caregivers or other significant supporting people”.
“Children and young people: For the purposes of this guideline: those aged up to 11 years are considered children; those aged from 12 to 24 years are considered to be young people”
Normalises gender diversity, normalises rise in referrals (UK GIDS describes the rise as ‘unexpected’ & speculates negative reasons for the rise)
“Internationally and within New Zealand there has been a substantial increase in the demand for gender affirming healthcare over the past decade. The Youth secondary school survey, estimated that approximately 1.2% of adolescents in New Zealand identify as transgender. It is likely that this level of referrals to health services will continue in the foreseeable future.”
Prioritises autonomy and avoidance of pathologisation (UK GIDS does not)
“Autonomy: Autonomy in the context of transgender healthcare involves transgender people being able to able to make informed choices for themselves regarding gender affirming care and being free from experiencing harmful pathologisation and other barriers to accessing this care.”
Acknowledges the importance of partnering with trans communities (UK GIDS does not)
“To successfully enhance the health and wellbeing of transgender people, providers need to partner with transgender communities to shape these services.”
Acknowledges that gender affirming healthcare is medically necessary (UK GIDS does not)
“The medical necessity of gender affirming healthcare has been acknowledged by WPATH, the Australian and New Zealand Professional Association for Transgender Health (ANZPATH) and many other international organisations.
The Yogyakarta Principles pull together existing international human rights legal standards which state that transgender people have the right to access the highest attainable standard of gender affirming care.
Acknowledges the impact of social stigmatisation including in the healthcare system (UK GIDS does not)
“Social stigmatisation and discrimination, including within the healthcare system, present additional barriers to accessing health services and contributes to adverse health outcomes”.
Prioritises community leadership (UK GIDS does not)
“Community leadership: This guiding principle informs us that for health promotion to be effective it needs to be led by relevant communities. Health professionals have important roles to play but cannot replace the leadership which exists in communities. An example of this is the partnership between transgender communities and the Northern Region health board from 2014 to present. Transgender people have been involved in the steering of the project, including development of services and these guidelines. The importance of trans community leadership in the development of trans healthcare services is paramount.”
Recognises the importance of different areas of health: (UK GIDS does not)
“Transgender health recognises the equal importance of spiritual health, family health, mental health and physical health.”
Acknowledges legacy of pathologisation of gender diversity and clarifies it is not a mental health illness, acknowledging the importance of avoiding stigmatisation (UK GIDS does not)
“Historically transgender healthcare has suffered from the pathologising of gender diversity and the inappropriate labelling of gender/cultural identity and expression as a diagnosed mental health illness. The resulting legacy of this pathologisation is a tension in health services between the need to avoid further stigmatisation while simultaneously acknowledging the importance of the wider concept of mental health as part of holistic healthcare delivery.”
Prioritises informed consent and self determination (UK GIDS does not)
“The practice of informed consent in relation to gender affirming healthcare is important because it reaffirms the self-determination of the transgender person and their knowledge of their needs, identities, and self. Informed consent enables the health provider to work alongside the transgender person in a flexible and responsive way”.
Recommends involving trans people in development and provision of services. (UK GIDS does not)
“Health services enable the involvement of trans and gender diverse people, including Māori trans people, in decisions that affect them with regard to the development and provision of services.”
Commits to improving based on feedback (UK GIDS does not)
“Health services have a process for receiving feedback and evaluating people’s experience that report on outcomes and commit to acting on the feedback/data received to improve services.”
Recognises impact of colonisation in persecuting gender minorities who were accepted and valued in pre-colonial society (UK GIDS does not)
“It is increasingly apparent that, in Aotearoa pre-colonial Māori society, people of diverse genders and sexualities were both accepted and valued within extended families. The colonisation in the 1800s by the British had a huge impact on Māori culture and society. Any expression of gender or sexual fluidity was strongly discouraged by the missionaries. Recorded histories overlooked or erased stories of takatāpui.
Likewise, Pacific cultures also accepted gender diversity as part of the normal range of human expression. The impact of colonisation of many of the Pacific Island nations through faith-based missions and colonial government administrations has had a negative impact on the acceptance of gender diverse people.”
Recognises the minority stress intrinsic to living in a transphobic society (UK GIDs does not)
“Tangata takatāpui moved from a social and cultural situation where minority stress was simply not a factor in the pre-colonial world of Māori, to one where it has become a key force in the negative health outcomes they experience”.
“Minority stress: Minority stress theory suggests that trans and gender diverse people experience stressors as a result of sociocultural sanctions about being transgender and/or gender nonconforming. These include prejudice, discrimination and violence which negatively impact on physical, social, spiritual, and psychological wellbeing. It is important to note that minority stress results from a multitude of everyday events that trans people experience. Daily stressors for trans people can include not being affirmed by health providers, being asked invasive questions in inappropriate settings, or not having access to a safe public bathroom. Minority stress here includes the economic stressors that many trans and gender diverse people also negotiate.”
Recognises that supporting wellbeing of trans people must include addressing these barriers to health (UK GIDS does not)
“Supporting the wellbeing of transgender people includes recognising that barriers to health, housing and employment will have negative health impacts. Improving health services is part of creating health, education, housing, and employment environments that are accessible, respectful, and inclusive of trans and gender diverse people”.
Recognises the importance of trans positive health services (UK GIDS does not)
“Trans positive health services: Primary and secondary health services that are respectful and affirming of people’s gender identities can have a positive impact on trans people’s well-being. There are many important nonmedical supports that can be useful for health services to be aware of when supporting people who are socially transitioning.”
Supports social transition (UK GIDS does not)
“Social transition: Social transition consists of the steps many transgender people choose to take to alter their presentation in the world to better align with their gender identity. Transition looks different for every individual and it is important to note that neither social or medical transition is required in order to be recognised as a trans or gender diverse person.
Transgender people should be supported through these steps of social transition to allow them to have positive experiences in the world as a truer representation of themselves. Social transition can also start out part-time in known safe environments, such as home or school.”
*Note there is nothing negative here about the psychological impact of social transition (GIDS latest scare story). There is no age-based barrier to support. No references to the discredited and harmful ‘watchful waiting approach’ that UK GIDS still clings to. Watchful waiting sounds benign. It depends what you are watching whilst you wait. For many trans kids, rejection causes immense harm. For many trans kids, affirmation and fully love and support allows our children to breathe, allows them to thrive, allows them to enjoy their childhoods. Why should trans children in New Zealand, Australia, USA, Canada, Spain (including Canary Islands) have happy childhoods whilst UK trans children are left depressed, rejected, ashamed.
Recognises family health (UK GIDS does not)
“Family Health: There are many forms of family support; a parent looking out for their trans child, an adult supporting their trans partner or parent through transition, a family advocating for respectful care of their trans relative in a resthome. In reality it is not just one person who ‘transitions’ but the whole family”.
Highlights that family support is a HIGHLY protective factor (UK GIDS does not)
“Family and young people: Family support is a highly protective factor for trans young people. Research shows that trans young people reporting strong family connectedness have a greatly reduced likelihood of poor mental health, even when experiencing stigma and discrimination elsewhere. Family support provides a place from which takatāpui rangatahi can draw strength and resilience to help deal with the challenges they face outside the family.”
Prioritises helping parents gain support to understand their loved one (UK GIDS does not)
“Parents report a range of emotions following disclosure from their child that they are transgender, including confusion, the need to have time to process, the need to grieve for the loss of a son/ daughter, fear for the future and acceptance of their child. While the young person is likely to have spent considerable time developing an understanding of who they are, families may perceive the change as being sudden and require time to adjust. Families report that they need information and time to understand their loved one’s journey. It is an important part of the role of health services to support this process. Some families find joining parent support groups helpful.”
Recommends primary and secondary health services provide clear, unambiguous affirmative advice to parents/carers (UK GIDS does not)
“Practice points: Primary and secondary health services need to provide education, promote connection to family and to support family to be able to support gender diverse children and young people through simple advice:
- Assure your child/young person that they have your unconditional love and support, or at least that you will commit to their journey with them.
- Encourage exploration of how they express themselves. It is important that young people have spaces in which they feel safe enough to explore their gender.
- Use the child/young persons preferred gender pronouns (he/him, she/her, they/them etc) and preferred name when they are ready to do so. Support family and friends to do the same, providing it is safe to do so.
- Provide written/online information for family.”
Is confident and non-pathologising on topic of transgender children (UK GIDS is not)
“Gender diverse children: Many children explore different ways of expressing their gender though play. Most of these children are comfortable with the sex they were assigned at birth, although some are not. Some children will assert themselves as a gender different from the sex assigned at birth. These transgender children are usually insistent, consistent and persistent in their gender identity and may exhibit distress or discomfort with their physical body. Some transgender children are aware of their gender identity from a very early age, while others may take some time to figure it out or find a safe way to express it. Children can be very aware of the disapproval of those around them and may try to hide their feelings about their gender. For gender expansive children, including those who may identify as transgender, no medical intervention is needed pre-puberty.”
*Note the way the language is affirming and reassuring about young trans children as well as affirming and reassuring about children who are aware of their identity later. The UK uses language that is unsupportive and un-reassuring about both.
Is clearly supportive of a gender affirmative approach for trans children, including unambiguous support for social transition (UK GIDS is not)
“Supporting trans and gender diverse children requires a developmentally appropriate and gender affirming approach which involves assisting children to create an environment where their gender can be affirmed. This might require providing education and support for families and schools to be able to support the gender diverse child to navigate a social transition and helping children to develop the coping skills to address any negative reactions that they might experience for being gender diverse. Family may want support from their primary care health team, a paediatrician, child and adolescent mental health service or parent support group to work out how best to support their child. This is particularly important if there is associated distress related to gender identity.
*note no fear mongering on social transition, no words of concern and caution, no words about regret or desistance, nothing on need to delay, deny or diagnose.
*note the emphasis on providing assistance externally, to make the world a better place for a trans child. The UK focuses their effort internally, onto the trans child themselves, focusing on psychoanalysis of that child, making their gender diversity the problem.
Non-pathologising about trans adolescents who are aware of their identity at puberty (UK GIDS is not)
“Young people: Trans young people may present to a range of health providers requesting support with their gender identity, so all health teams need to be able to provide an inclusive environment where young people will feel safe talking about their gender. Some young people present with longstanding diverse gender identities since childhood, while others find that adolescence was a crucial time for the development of their gender identity. Identity may emerge during or after the onset of the physical changes brought on by puberty and the changing social and romantic interactions with peers.
*note no scaremongering about social contagion. No scaremongering about adolescents confusing gender for sexuality. No scaremongering about social media and the influence of the internet. No undermining of the validity of trans teens who become aware of their identity at or after puberty (all of these have been talked about in the media by UK GIDS).
Non-pathologising understanding of gender fluidity (UK GIDS is not)
“Similarly, some previously gender expansive children may shift along the gender spectrum to find their gender identity more aligned with the sex assigned at birth. In all of these situations, these young people and their families will benefit from supportive healthcare providers who pay attention to how the young person is expressing their gender.”
*Note the guidance sees no trade-off or tension between supporting trans kids and supporting kids who shift gender modality. It argues that both benefit from supportive healthcare. UK GIDS likes to argue that their known harm to trans kids somehow benefits kids who might shift gender modality (despite no evidence of this).
Focuses on co-existing concerns without using co-existing concerns as a pretext for denying identity or delaying affirmation (UK GIDS does not)
“Trans young people need to be assessed routinely for risks around abuse, bullying, drug and alcohol use, nutrition and unhealthy eating behaviours, sexual health and any mental health concerns“
*It would not be surprising to me if youth with co-existing issues are better able to address other co-existing issues, once their gender is affirmed. In the UK adolescents with co-existing concerns are denied affirmation of their gender, on the pretext that their gender issues may be symptoms of a misguided coping strategy for dealing with other issues. There is no evidence for this approach which is rejected elsewhere and causes harm to some of the most vulnerable youth (eg descriptions of children and teens in UK GIDS having their identity invalidated and being forced to discuss trauma as a potential cause of gender ‘confusion’ if they have suffered abuse or bereavement).
Prioritises peer support (UK GIDS does not adequately encourage peer support and some media engagement has encouraged scaremongering on ‘social contagion’, discouraging wary parents from helping their child connect to peer support)
“Trans young people often benefit from being linked into supportive peer groups, including online groups.”
Understands trans kids may find puberty difficult (UK GIDs recent media engagement seemed to suggest that trans kids were finding puberty difficult because of being too supported and affirmed in their childhood – they suggested childhood rejection was the best way to avoid trans kids worrying about puberty)
“Anticipation of and/or experiencing pubertal body changes can be very distressing.”
Is clear and unambiguous on evidence of benefits of puberty blockers and gender affirming care (UK GIDS is not)
“There is good evidence that puberty blocking and gender affirming care for trans young people significantly improves mental health and wellbeing outcomes.”
When parents are unsupportive, unequivocally prioritises the need of trans adolescents, even under age 16 (GIDS does not)
“Decisions regarding medical interventions are ideally made collaboratively between the trans young person, their family and the health team. However, it is not always possible to involve family. Lack of family support does not preclude trans young people from accessing care. While young people aged 16 years and older are considered to be able to make decisions about their medical care younger people are not prohibited from consenting to medical interventions if the young person is deemed to be competent to make an informed choice. To assist this informed consent process, we recommend that gender affirming healthcare for young people is provided within a multi-disciplinary team”.
Prioritises the importance of trans students being in school (UK GIDS does not. In UK, the number of trans children out of school (often due to mental health problems linked to continued rejection, minority stress, violence, bullying) should be a national scandal)
“Schools: Feeling connected to school is also a significant protective factor for trans young people. Schools have an obligation to provide safe environment for their students. The Youth New Zealand school survey found that while 74% of trans young people thought that school was okay, 54% were afraid that someone at school would hurt or bother them. There are a range of support materials available for schools.”
Clearly is on the side of trans students and unambiguously supports the need for records to correctly reflect gender identity (UK GIDS does not)
“However, many students have reported to us that they still experience barriers to updating school records to correctly reflect their gender identity and experience gender-based exclusion from activities such as joining sports teams, choirs and groups”.
Recommends schools provide information on gender affirming healthcare (UK GIDS does not)
“Practice points for school health teams • Have information on gender affirming healthcare services readily available and on display. • Provide training on working with transgender students for the whole student health team”.
*UK language from GIDS to schools can be the opposite of affirming, referring to complex cases, pathologizing and stigmatising gender diversity and discouraging schools from full support.
Is interested in the general wellbeing of trans students (UK GIDS focuses on gender identity, is not proactive on discrimination)
“School health teams should: “• Have information and support available for transgender students who experience discrimination from students or teachers. • Be connected to local health and social services in your area that specialise in working with transgender young people. • Enable students to establish a diversity group or other support for transgender students (if they desire to do so).”
Provides clear affirmative guidance for family members: (UK GIDS does not)
“• Listen first and foremost. Be available to listen to your family member’s experiences. Make an active effort to listen without judgment. Remember that advice isn’t always necessary; sometimes all they need is a kind ear. • Respect trans people’s pronouns Trust that they are making the right decisions for themselves. • Educate yourself and others”.
Recommends family members listen to and learn from trans people (UK GIDS does not)
“Read and listen to the stories of transgender people. This will give you a better understanding of their experiences and enable you to interact in a positive way with your family member.”
Encourages peer support (UK GIDS does not)
“provide easily accessible information and access to peer support services for trans people of all ages and their family”.
Recommends children receive gender affirming healthcare (UK GIDS does not)
“That gender affirming healthcare services for children and young people are provided by clinicians with expertise in child and youth development.”
*note there is no requirement for psychoanalysis, the foundation of the UK GIDS service.
Non-pathologising approach to mental health of trans people (UK GIDS does not)
“Mental health: Trans and gender diverse people have the same inherent potential to flourish and thrive as other people, but currently experience increased risk of harm because of discrimination, social exclusion, bullying and assault, as well as institutional barriers such as difficulties accessing healthcare, bathrooms, and appropriate legal identification. Trans people from ethnic minority or refugee backgrounds are likely to be at even greater risk of experiencing harm.”
*GIDS does not acknowledge that trans kids have the same inherent potential to flourish and thrive. It does not acknowledge that the mental distress trans kids face is in large part due to cisnormativity and transphobia, including in (and encouraged by) NHS health services.
Acknowledges wider determinants of health (UK GIDS does not)
“It is becoming increasingly accepted that it is the additive effects of minority stress that results in mental health difficulties. It is important that health services acknowledge these wider determinants of health and the potential role they play in leading positive societal change to improve health outcomes”.
*The best things NHS GIDS could do for trans children is to give clear unambiguous affirmative trans positive statements about trans children to schools, to parents, to the UK media. Instead they do the exact opposite, making life so much harder – literally making minority stress and wider determinants of health worse. Where is the commitment to Do No Harm when it comes to the NHS and trans children?
Explicit on benefits of affirmative care on mental health and wellbeing (UK GIDS does not)
“Being transgender is often but not always accompanied by gender dysphoria, a person’s discomfort or distress with their body or gender roles associated with their sex assigned at birth. Constant reminders can be experienced when showering or dressing. However, increasing evidence demonstrates that supportive, gender affirming care for trans people significantly improves gender dysphoria and mental health and wellbeing outcomes. International studies consistently show high rates of mental health issues such as anxiety and depression for trans people. In New Zealand the Youth’12 secondary school survey highlighted the mental health disparities experienced by transgender young people compared to their cis gender peers with 41% vs 12% experiencing significant depressive symptoms and 20% vs 4% reporting an attempted suicide, respectively, in the past 12 months. Because of the high prevalence of mental health problems among trans people, health services that are multidisciplinary and include mental health professionals will be more responsive to the on-going needs of trans people accessing gender affirming health care.
Psychotherapy is not mandatory (psychoanalysis is integral to UK GIDS)
The role of mental health professionals: Trans people may seek support from mental health professionals for a range of reasons, including support related to their gender or concerns with their mental health. Mental health professionals should be aware that mental health problems may be related to the effects of minority stress for being transgender or may be due to other causes. While many trans people access psychotherapy for support with living in their affirmed gender, psychotherapy is not a requirement of accessing gender affirming care. Mental health professionals with the appropriate skills and knowledge can assist with the informed consent process for readiness for gender affirming hormones. The WPATH SOC state that it is important for mental health professionals to have open dialogue with prescribing practitioners, and other providers of a trans person’s care and to access regular peer consultation and feedback. These mental health professionals should have the knowledge to provide information to trans people regarding gender affirming care treatment options and community support availability”.
Recognises the duty of health service providers to be an advocate for trans people (UK GIDS absolutely does not)
“Finally, an important component of ethical health care provision is for providers to be advocates for the trans people who use their services. This could include educating or working with family members, schools, workplaces, healthcare settings, and other parts of the community on being inclusive and affirming of trans people. Recognising stigma, discrimination, and violence as the source of many issues that trans people face in Aotearoa, New Zealand, all health professionals should work collaboratively with trans people to advocate for social and public policy change to reduce the negative effects of minority stress”.
Mental health issues are not a barrier to gender affirmative care (In UK GIDS they are)
“Practice points • Include mental health issues as part of a holistic psychosocial assessment, for example discussion of anxiety, depression, risk of self-harm, while being clear that having mental health issues is not a barrier to accessing gender affirming services. • With the involvement and consent of the transgender person, plan for provision of on-going support for any mental health issues identified. • Respect the self-determination of each person as being the expert on their experience. This is often referred to as the “informed consent model” of gender affirming healthcare because it counteracts pathologisation and repositions the transgender person as being at the centre of their own life. • Recognise the impact of hostile environments on trans and gender diverse people, (i.e. minority stress) and validate the experiences that people have navigating those environments. • Ensure access to gender affirming health services alongside secondary mental health services: provide clear information about what to expect from secondary mental health services if referrals are appropriate, and work alongside secondary mental health services if they are involved”.
Recognises that trans children/young people may want support with challenges that are not related to gender (UK GIDS forces a prolonged focus on gender as the problem)
“When discussing stressors, follow the transgender person’s lead as to whether their current challenges and health needs are focused on their gender or on something else in their life. • Listen to each transgender person about ways that they would appreciate you advocating for them, which may be on an immediate interpersonal level (for example with family members or other health providers) or on a broader level in relation to other settings such as schools and workplaces”.
Embeds guidance for trans children in guidance for trans people of all ages (UK GIDS keeps trans children separate – using this to maintain a greater degree of pathologisation than would be accepted in adult care). Eg this section on pronouns is written the same for adults or children. Children are not treated worse just because they are young.
“Listen and reflect back the language each person uses about themselves, including gender identity terms, preferred names (even if not legally changed) and correct pronouns”.
Recognises neurodiverse people can also be trans (UK GIDS raises extra barrier to care for neurodiverse children and young people. In the media and to parents UK GIDS emphasises neurodiverse children and young people may be confused about gender identity)
“Neurodiversity and gender diversity It has been increasingly recognised that neurodiversity (autism spectrum) is common among the transgender community. Involving clinicians with the relevant diagnostic skills can be helpful for some people, as being able to identify as being on the autism spectrum can be helpful to understand behaviour and learn strategies to manage any difficulties. It is important to acknowledge that the person presenting is the expert on their own experience. Although some neurodiverse people may have difficulty in articulating their gender identity, this should not create an unnecessary barrier to access any relevant gender affirming services. Some people may express their gender identity non-verbally. The presence of neurodiversity can add complexity and extra time and support may potentially be required to help navigate all stages of the gender health journey including gender exploration, social, medical and surgical transition. Family may need support to understand more about the co-existence of neurodiversity and gender diversity, so that they understand that it is a common overlap and that being on the autism spectrum does not invalidate being transgender or seeking health services as part of transitioning.”
*See how reassuring the language is above. We never hear this from UK GIDS, who encourage allistic parents to reject neurodiverse children’s gender identity (for insistent trans children, the euphemisms that UK GIDS uses to avoid accusations of conversion therapy ie ‘delay’ ‘caution’ ‘watchful waiting’ equals rejection in practice).
“It is recommended that clinicians consider two key questions when working with people on the autism spectrum: • Is the gender identity clear, urgent, pervasive, and persistent over time? • Does the gender dysphoria increase or decrease with interventions?”
Physical Health is dealt with alongside wider health dimensions (UK GIDS focuses on psychoanalysis to test/validate gender identity followed by physical interventions)
“The physical dimension is just one aspect of health and well-being and cannot be separated from the aspect of mind, spirit and family. These guidelines are based on the principle of trans people’s autonomy of their own bodies, represented by healthcare provision based on informed consent.”
Prioritises informed consent (UK GIDS does not)
“Medical treatments such as hormone therapies and surgical interventions may also be an important part of a person’s transition and physical health. While many trans people will benefit from hormone therapies and surgical interventions, some may choose only one of these options and others may decide to have neither. For those who are seeking medical support, access to competent care through an informed consent model is of paramount importance.
In regards to transition goals, it is important to recognize that each person will articulate these differently. It is not helpful to assume that everyone wants to conform to binary gender norms and clinicians need to be aware not to impose a binary view of gender.
The importance of discussing individual transition goals and individualising treatment options is especially true for non-binary people but also applies to those with a more binary gender”.
States unambiguously that withholding gender affirming treatment is not a neutral option (UK GIDS does not)
“Withholding gender affirming treatment is not considered a neutral option.
Avoiding harm is a fundamental ethical consideration for health professionals when considering healthcare. Withholding gender affirming treatment is not considered a neutral option, as this may cause or exacerbate any gender dysphoria or mental health problems. Conversely, access to gender affirming care may reduce the mental health pressures a trans or gender diverse person is experiencing. This does not discount that clinical decisions can be complex, particularly where there is family opposition for young people, the person is neurodiverse or has complex mental health needs. It is best practice that gender affirming healthcare is provided by well-resourced multidisciplinary teams that include mental health professionals and have good links with peer support groups.
Practice points: Acknowledge that withholding gender affirming healthcare is not considered a neutral option”.
Being trans and wanted to socially transition is not a mental health condition, mental health support should be optional not mandatory (in UK GIDS it is mandatory and indeed at the heart of their approach)
“Social transition can be a stressful time for some people who may benefit from extra mental health support, but it is important to ensure that they consent to having this support and it is not enforced as a requirement for accessing gender affirming care.”
Emphasises that much can be done in primary health care (UK GIDS continually communicates how specialist and complex everything linked to trans children and young people is)
“Accessible gender affirming care involves people being able to access this care as close to home as possible. There are limited numbers of teams that are specialised in gender affirming care in New Zealand and these are receiving increasing demand. Primary health providers should be aware of the barriers and potential harms with requiring people to travel or wait to access care and might consider assessment and provision of gender affirming hormones within the primary care setting.”
Emphasises clearly and confidently the positive impact of puberty blockers on wellbeing (UK GIDS does not talk in the below terms about puberty blockers)
“Puberty suppression using GnRH agonists: Health teams need to be aware of the positive impact of puberty blockers (GnRH agonists) on future well-being. Be mindful of the need to refer promptly and be aware of referral pathways. Puberty blockers can be prescribed from Tanner stage 2 to suppress the development of secondary sex characteristics, although are still beneficial when prescribed later in puberty to prevent ongoing masculinisation/feminisation. Puberty blockers are considered to be fully reversible and allow the adolescent time prior to making a decision on starting hormone therapy. They do not stop growth or weight gain, and monitoring of height is recommended as adult height may potentially be increased if prolonged puberty suppression delays epiphyseal fusing. A bone age may be helpful to assess whether epiphyseal closure has occurred when considering what rate of hormonal induction to use as this may potentially impact on final height. Puberty blockers halt the continuing development of secondary sexual characteristics, such as breast growth or voice deepening, and relieve distress associated with these bodily changes for trans young people. For trans women and transfeminine people, they will prevent further masculinisation of the face and body that typically occurs into early adulthood.
*Note how confidently New Zealand health guidance talks about puberty blockers. GIDS does not talk in such reassuring ways about puberty blockers. GIDS instead speculate on an unevidenced theory about blockers potentially affecting brain development in mysterious and unstated ways. Brain development! This sounds really scary! But actually it is fully unscientific and vague – the kind of speculation you get from psychoanalysis who are not medically qualified. Do you think paediatricians go around speculating (with zero evidence) to parents about the irreversible impact on brain development of a drug that they have just prescribed to a cis 12 year old? They say ‘we don’t fully know the impact of them on adolescent brain development’. They also say things like ‘they are not reversible, as if you have taken them, you won’t know what it is like to have never taken them’. Well no shit sherlock but that isn’t what we are talking about when we talk about whether or not drugs are reversible. They also basically say to parents ‘there’s no evidence’ and ‘we give these blockers out but we don’t know what we are doing or if maybe it is the wrong thing to do’. Some anti-trans clinicians are known to tell parents that they believe blockers are harmful. Goodness me – no wonder there is so much hysteria in the UK on trans children’s healthcare when the NHS is telling parents and media that it is prescribing drugs it does not have confidence in. The way in which UK GIDS communicates about puberty blockers is an indication of the systemic transphobia in UK GIDS – it causes real harm and negative health outcomes for trans children and families.
Access to gender affirming hormones on an individualised basis (not possible in UK GIDS)
“Gender affirming hormone treatment. In New Zealand young people aged 16 years and older are considered to be able to consent to medical care (Care of Children Act 2004), however it is increasingly recognised that there may be compelling reasons to initiate hormones prior to the age of 16 years for some individuals, although there is as yet little published evidence to support this. Consideration should be given to the individual circumstances including family support, length of time on blockers, concerns around final height, risks of delaying hormones and most importantly the ability to consent”.
Having mental health concerns is not a barrier to affirming care (It is in UK GIDS – being out of education (eg due to schools being able to tackle transphobic bullying, being depressed etc is a barrier to accessing HRT in UK GIDS)
“The WPATH standards emphasise that the having medical or mental health concerns does not mean gender affirming care cannot be commenced, rather that these need to be responded to alongside gender affirming care. According to the standards, this readiness can be assessed by a prescribing provider or mental health professional who is experienced and competent at working with trans people.”
*Who gets to decide the definition of ‘competent at working with trans people? Would anyone in UK GIDS pass? I have heard of maybe three clinicians out of 60+ who people have regularly positive feedback on.
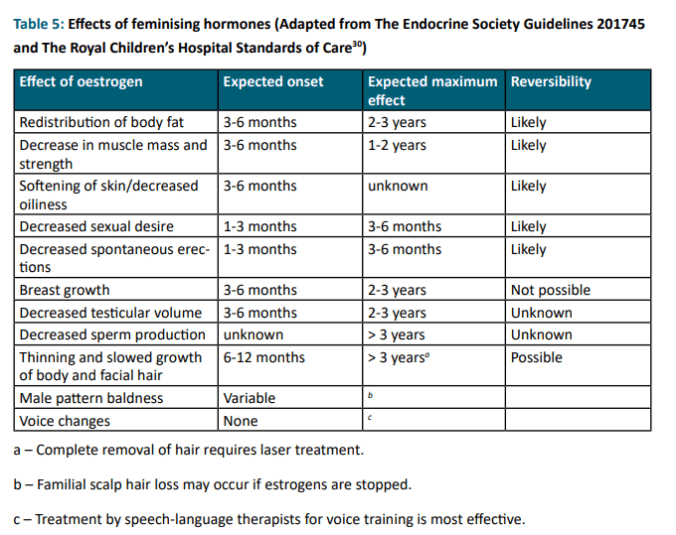
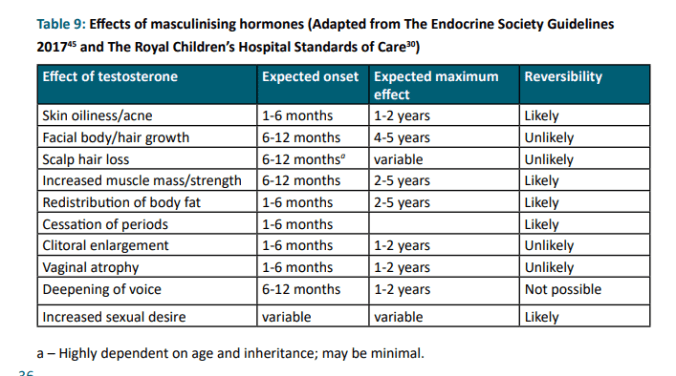
Clear, reassuring, easy to understand communication on the effects of masculinising hormones or feminising (GIDS does not provide it so clearly for public understanding)
Fertility
I’ve not much considered the sections on fertility in this blog as a bit off my main focus. But two bits stood out. There is an Annex B on fertility information. I wasn’t clear whether this leaflet is accurate for those who have had blockers at Tanner stage 2 and never progressed beyond Tanner 2 of the puberty associated with their assigned gender?
Consent for form blocking testosterone is very clear, confident and reassuring, and also includes information on the harms of NOT blocking testosterone
“Annex C: A consent form for blocking ‘male’ hormones”.
Includes clear language on common side effects
“• Hot flushes • Mood swings – mostly in the first few weeks of starting • Possible fatigue. Most side effects should settle within a few days to weeks of starting the medications. Allergic reactions can happen but are rare. Please tell your health team if you have any problems. Potential risks of blockers • Increased height (unlikely if already through puberty) • Decrease future bone density”
Also includes:
“Risks of withholding blockers: Withholding the use of blockers may cause additional distress leading to anxiety and depression. Not using blockers can also lead to irreversible unwanted physical changes”.
Interesting mention of need for contraception whilst on blocker, is this included in UK guidance?
Consent for form blocking oestrogen is very clear, confident and reassuring, and also includes information on the harms of NOT blocking oestrogen
“Annex D; A consent form for blocking ‘female’ hormone”.
“Blockers are a reversible medication used to stop the physical changes of puberty. It can be started in early puberty (Tanner stage 2–3). If started then blockers will usually stop significant breast development and further pubertal changes such as starting periods and widening of the hips. Blockers can also be started later in puberty where it may cause breast tissue to soften but not usually to reduce significantly in size. Blockers will stop periods but may take up to 3–6 months to do so
Starting a blocker often improves psychological distress associated with having the unwanted female hormone and allows time to think about whether starting testosterone is right for you.
Common side effects
- Hot flushes • Mood swings – mostly in the first few weeks of starting • Possible fatigue. Most side effects should settle within a few days to weeks of starting the medications. Allergic reactions can happen but are rare. Please tell your health team if you have any problems. Potential risks of blockers • Increased height (unlikely if already through puberty) • Decrease future bone density”.
Also mentions:
“Risks of withholding blockers: Withholding the use of blockers may cause additional distress leading to anxiety and depression. Not using blockers can also lead to irreversible unwanted physical changes”.
