The heads of the UK Children’s Gender Identity Service (GIDS) have just published a new journal article, featured in the British Medical Journal ‘Archives of Disease in Childhood’:
“Assessment and support of children and adolescents with gender dysphoria” Gary Butler (Consultant Paediatric Endocrinologist), Nastasja De Graaf (GIDS researcher), Bernadette Wren (Head of Psychology at GIDS), Polly Carmichael (GIDS Director).
This latest article from the heads of the UK children’s gender service (GIDS) sets out the UK service’s position and deserves close scrutiny. Here goes:
Introduction
The article is intended for “professionals” who:
“may be unsure how best to provide supportive care, how to access the national Gender Identity Development Service (GIDS) for children and adolescents, or how to deal with a transgender young person presenting with another clinical problem unrelated to their gender transition”
Referencing fringe figures
The first reference they have chosen to include is co-authored by Ray Blanchard and Kenneth Zucker, two controversial figures, the former whose theories have been rejected by mainstream practitioners and who is known for speaking about trans people with disrespect, and the latter who was sacked from his clinic in Canada for work that could not be distinguished from conversion therapy and who has compared trans children to animals.
Conflating behaviour with identity
For a guide intended for non-specialists, the publication from the very start confuses and conflates behaviour, expression and identity:
“Gender atypical behaviour is common among young children and can be part of general development”.
They omit any publications (e.g. Hidalgo et al 2013, Olson et al 2015, Ehrensaft 2016, Fast & Olson 2017) that evidence the existence of trans children at a young age – with an insistent, consistent, persistent gender identity different from the one assigned at birth. They also omit to mention that trans children may or may not have non-traditional behaviour or expression. Gender identity and behaviour/expression are different things, and any publication intending to educate, should be clear on this. This omission is a fundamental failing.
Focus on exponential rate of rise, not on actual numbers compared to population prevalence
The first paragraph focuses on the ‘exponential’ rise in referrals since 2011. The language is alarmist, with the focus only on the rate of increase, with no discussion of the actual numbers. The actual numbers are extremely low and as with all low numbers, can easily show exponential growth.
The section on prevalence contains no discussion on how these low actual numbers compare to estimates of prevalence across the population. There is an alarmist focus on the growth rate without mentioning the numbers for 2011 were only 200 children a year (from the UK population of 60 million) and in 2016 were only 2,000 children a year. 2,000 children a year from a under 18 population of about 14 million children in the UK is still a very small percentage. So yes from 200 to 2000 is an exponential rise, but it is still only a tiny fraction of the under 18s in the UK.
This section does not mention that recent population prevalence surveys have put the trans population at around 1%, which would mean up to 140,000 of those currently under 18 might identify as trans. Referral numbers rising from 200 a year to 2,000 a year should not be a surprise in this context.
There is also zero discussion of the wider context, not only the rise in visibility and awareness of trans people in general, but the specific context in the UK – GIDS mentions a rise in referrals since 2011 with no mention of the arrival of the Equality Act in 2010, legislation that protected trans children and enabled families like mine to feel safe enough to get support at school and in other areas – protection that allowed families to be more open, protection that enabled families to support their child.
Australian gender specialists describe a rise in referrals in a completely different manner:
“Spurred on by increasing acceptance of transgender individuals in society (and normalisation of the right for anyone to question their gender identity), the number of young people seeking support is likely to increase further”
UK GIDS cannot seriously claim the rise in referrals is unexpected – a rise in referrals was predicted by GIRES back in 2009.
Focus on rise in ‘birth registered females’
GIDS continue:
“A striking feature of this increase is the large proportion of birth-registered females from 2011 onwards. This increase and the change in sex ratio is also seen in other countries.
Let’s break this down. Again the focus on rise in referrals. From 57% assigned female in 2011 to 69% assigned female in 2016. From about 100 assigned females in 2011 to about 1,400 in 2016, from a population of 64 million people in the UK. Any analysis of trans prevalence would acknowledge that the 100 referrals of assigned females under 18 years old in 2011 was a gross under-representation. A rise in assigned female referrals was predicted by GIRES in 2011. A less transphobic service would celebrate the fact that more assigned females are getting listened to, getting referrals and getting support.
The Fig for the accompanying graph states “referrals by birth-registered gender”. In the UK birth certificates state ‘sex’ not ‘gender’. GIDS should be aware of this.
Here appears the second academic reference in their paper. The first was co-authored by Zucker and Blanchard. Who is their chosen second reference? Oh, of course, it is another paper co-authored by Zucker.
Inclusion of unsubstantiated speculation
“The reasons (for rise in assigned females) are not fully explicable and a number of questions arise. Is this increase due mostly to the greater tolerance of gender-diverse expression in westernised society? Is male status still regarded as preferable?“
We are still in the paper’s first proper paragraph, in a paper intended to educate professionals, who are not gender specialists, in evidence based medical consensus. At this point in the paper, GIDS decides it is appropriate to engage in unevidenced speculation about the reason for a rise in assigned females. It chooses to include unevidenced speculation that matches a fringe theory proffered by transphobic lobby groups: “Is male status still regarded as preferable?”.
This unqualified speculation implies that children and adolescents are choosing to be trans. That trans boys choose to be trans to benefit from the enhanced status that comes with being seen as a trans boy. This suggestion woefully minimises the very real challenges facing trans boys and trans masculine children in a transphobic UK. But most importantly it is not supported by evidence. This is a GIDS publication in a medical journal. Do NHS professionals in medical journals routinely apply speculation on medical care eg. for reasons for a rise in asthma? Why are professional standards for trans children’s medical professionals so dire?
And more:
“What are the benefits, as well as the possible harms, in supporting and helping these young people at different stages of development?”
GIDS are not talking about the nuances of different treatment pathways here – they are saying that ‘supporting and helping’ young people has the potential to cause harm. Implying that there are circumstances when it is better to not ‘support’ and not ‘help’ young people.
Noticeably, despite extensive evidence of the harms of withholding care to trans adolescents (See Giordano and here ), they choose not to include any reference to the known harms associated with not helping young people. The then Chair of the NHS Clinical Reference Group for Gender stated that “not treating people is not a neutral act. IT WILL DO HARM”.
“Not treating people is not a neutral act. It will do harm: there are a number of studies that report evidence of suicide and self-harm among trans people who are unable to access care.”
John Dean, MBBS, FRCGP, Chair, National Clinical Reference Group for Gender
Identity Services, England
Here is the 2017 Australian Standards of Care for trans children (now also published in the Lancet) on withholding treatment:
“Avoiding harm is an important ethical consideration for health professionals when
considering different options for medical and surgical intervention. Withholding of
gender affirming treatment is not considered a neutral option, and may exacerbate
distress in a number of ways including increasing depression, anxiety and suicidality,
social withdrawal, as well as possibly increasing chances of young people illegally
accessing medications”.
GIDS omits any reference to evidence that withholding care causes harm.
Criteria for the diagnosis of Gender Dysphoria
GIDS describe the diagnosis of Gender Dysphoria (from the 2013 DSM-5) and focus on descriptions of behaviour.
There are many problems with the DSM-5 diagnostic criteria that GIDS are either unaware of, or choose not to discuss.
Contrast this with the astute approach Johanna Olson-Kennedy takes to DSM-5 gender dysphoria diagnostic criteria.
Dr. Olson-Kennedy critiques the adult Gender Dyspohria diagnosis that requires a trans person to have “a strong conviction that one has the typical feelings and reactions of the other gender”. Olson-Kennedy ridicules this describing her “big book of typical feelings and reactions, the blue pages are male and the pink female”.
The DSM-5 gender dysphoria diagnostic criteria for children is even more absurd. In order for a child to be diagnosed with gender dysphoria, they HAVE to say yes to at least one of these three outdated, stereotyped criteria:
-
A strong preference for the toys, games or activities stereotypically used or engaged in by the other gender.
-
A strong preference for playmates of the other gender.
-
A strong rejection of toys, games and activities typical of one’s assigned gender.
If a trans child such as mine, likes a wide variety of toys and plays with all children (and how can that possibly be a bad thing?) then that child CANNOT be diagnosed as gender dysphoric according to DSM-5. The diagnosis is obviously nonsensical.
It is a stereotyped and confused mess of a diagnostic tool, yet the GIDS paper presents this without critique, qualification, or apology, instead accepting and endorsing its focus on behaviour rather than identity. Perhaps this endorsement is because GIDS are content with a confusion between gender identity and behaviour – confusion that is consistently used by vocal transphobic lobbyists to argue against support for trans children.
The GIDS article states: “for children, cross-gender behaviours may start between the ages 2 and 4, the same age at which most typically developing children begin showing gendered behaviours and interests”.
Why are they focusing on behaviour and interests? If the authors had any understanding of gender, they would examine how and why behaviour and interest do not equal identity. This omission is astonishing.
Again, no mention of Olson 2015 or Fast 2017 that found: “Transgender children do indeed exist and their identity is a deeply held one” providing evidence that “early in development, transgender youth are statistically indistinguishable from cisgender children of the same gender identity.” This research literature from the US is completely omitted from the GIDS paper.
Do GIDS feel it is appropriate to disregard academic literature that challenges their (unevidenced) beliefs?
The language contrasting trans children with ‘typically developing children’ is also cisnormative and pathologizing. My child is developing typically. She just happens to be trans.
Cisnormative and outdated terminology
GIDS include a glossary of ‘useful terminology’. The definitions they have chosen to use, and those that are missing, evidence their cisnormativity and lack of sensitivity or awareness of trans inclusive language and risk alienating their service users.
“Transgender: Transgender refers to the broad spectrum of individuals who identify with a gender other than that associated with their birth sex”.
The phrase ‘birth sex’ is outdated – ‘assigned sex’ is used for a reason. Especially given the 2017 Endocrine Society guidelines has a whole section on the substantial evidence of a biological underpinning to gender identity (something GIDS do not reference in their paper).
Here’s a better definition, from the Australian Standards of Care: “Trans/Transgender: A term for someone whose gender identity is not congruent with their sex assigned at birth”
“Non-binary: Non-binary is a lack of identification with conventional maleness or femaleness. Non-binary people may express features of both genders or neither.”
This muddled definition places more emphasis on gender expression than on identity. It is also ironic, in a definition of non-binary, to use the phrase ‘both genders’. A better definition would focus on identity not expression: “Non-binary: A term to describe someone who doesn’t identify exclusively as male or female”.
“Transman/transboy: A person born phenotypically female (natal female), registered (assigned) female at birth, who identifies as male. Also known as female to male.”
Many trans people consider the lack of space between trans and man or boy offensive. Trans is an adjective. ‘Transman’ is a term frequently used by those who wish to other trans people. It is used by those who argue that trans men are not men. The definition is also cisnormative – the phrase ‘identifies as‘ would never be used for a cis man.
The GIDS definition of a ‘transman’ states ‘a …female….female….female who identifies as male’. The term ‘female’ appears three times in their definition before the word male.
Further, the term ‘natal female’ is widely considered outdated and offensive by trans people. The Endocrine Society states there is clear evidence of a biological underpinning to gender identity. Trans boys are not ‘natal females’. Many medical professionals already use gender affirming terminology, with even the Endocrine Society using the term transgender male to refer to trans men – there is simply no justifiable reason to use the term ‘natal female’ when talking about trans men.
“Transwoman/transgirl: A person born phenotypically male (natal male), registered (assigned) male at birth, who identifies as female. Also known as male to female.”
As above – where is the space between trans and woman or ‘girl’? ‘Transwoman’ is a term used by those with deep seated hostility to trans women to attack and discriminate. It is considered by many to be deeply offensive. Are the authors so unaware that this language is deprecated?
Again, in their definition of a trans woman (transwoman), they repeat the word male three times before saying ‘who identifies as female’.
The text suggests that the term ‘male to female’ is a noun and a synonym for trans girl. Not helpful.
Cisgender
GIDS do not include a definition of the word cis or cisgender. The words cis or cisgender are not used ONCE in their paper. Through these definitions and omission GIDS erase and ‘other’ trans people and their service users.
Appropriate assessments prior to referral
“The GIDS is an unusual multidisciplinary service in that the initial assessment … is aimed at understanding the young person’s development and gender identification in the context of their family background and life experiences It takes account of how they feel about their gender and their body now and in the past, the context in which the gender dysphoric feelings arose and intensified, how these feelings are being managed in everyday life, and what hopes are held for proceeding in the future”.
GIDS focus is on ‘the context in which the gender dysphoric feelings arose’. They place causation at the centre (a later section of the paper discusses their quest for a diagnostic test for ‘transness’ – asking a child their identity apparently didn’t occur to them.
There is no discussion of the 2016 Lancet publication which states that parenting has no impact on gender identity. There is no mention that gender identity is resilient to external influence, and no mention that past attempts to externally change a gender identity are considered unethical and ineffective. These omissions are damning.
Compare the Australian standards of care which explicitly covers those issues which are ignored by GIDS:
“In the past, psychological practices attempting to change a person’s gender identity to be more aligned with their sex assigned at birth were used. Such practices, typically known as conversion or reparative therapies, lack efficacy, are considered unethical and may cause lasting damage to a child or adolescent’s social and emotional health and wellbeing”.
Autism
“Around 35% of referred young people present with moderate to severe autistic traits”.
GIDS provide no published detail, nothing of their methodology and no discussion of the number of children who have ‘moderate’ versus ‘severe’.
This sentence also smacks of ableism. The statistic about autism is given without any discussion of how their service supports and cares for neuro-diverse trans children. For a brief summary of current literature on the intersections of gender diversity and autism see this 2017 review by Gender Analysis.
Assessment
“The assessment period usually takes 6 months or more over a minimum of four to six sessions”.
Earlier in this paper GIDS have already confirmed that they follow the NHS service specification. Their own service specification clearly states on page 13:
“an initial assessment process which will be specific to the person in terms of duration and will typically be over three to six meetings depending on the individual”.
GIDS’ own service specification commits to individualised care, yet here they are stating a minimum of four sessions regardless of circumstance. In a service where waiting lists for a first appointment (once a family manage to secure a referral from a GP) have risen to 18 months!
These illegal and unethical waiting periods have a direct negative impact on young people and their families. There are reports of families re-mortgaging homes to afford private care outside of the UK. There is a growing practice of (dangerous) self-medication. These problems are entirely avoidable and are a direct consequence of a lack of individualised care and the appalling waiting lists created as a result.
Trans teens are a highly vulnerable group – making a highly distressed trans teen entering puberty wait 18 months for a first appointment and then inflict an inflexible protocol requiring a minimum 4 sessions, spread months apart, before any consideration of a referral (with further assessment and delay) to the endocrine service, for fully reversible, safe, puberty blockers, is both unnecessarily CRUEL, and a gross dereliction of duty of care.
“At the end of the assessment, it may be possible to confirm or exclude a diagnosis of GD”.
Note the arrogance and where the power lies. The clinician can ‘exclude’ a diagnosis of Gender Dysphoria. There is no practical recourse, no appeal, and no power to challenge the monopoly service authority over trans children.
Rates of referral to pediatric endocrine clinic
For several years GIDS have been talking about rates of continuation to medical intervention, without ever providing any published data.
Head of service Polly Carmichael spoke on the Victoria Derbyshire Show on the 7th August 2017:
Polly was asked by the presenter Victoria Derbyshire:
“How often might you see a child at a young age, 3 or 4 or 5 who as they grow or mature eventually change their mind?”
Polly answered:
“Those that are referred to the service at 5 years old it will only be 6% of those who ultimately go on to seek physical interventions to change their body”
Following this national media appearance parents asked GIDS to SHOW US THE DATA.
Radio silence. GIDS confidently, publicly, state a statistic about a specific group (only 6% of 5 year olds will go on..) on national television, ignoring the negative impacts this may have on families with trans children, and then fail to publish anything to support their claim.
This is a gross abuse of their power.
For years parents have been asking GIDS to publish data to support claims that they have been stating on national television morning breakfast shows, in newspapers, at medical conferences. These claims that are interpreted by viewers and readers as exceedingly high rates of children ‘changing their minds’.
Finally, in this paper, GIDS have included data, and within the respected British Medical Journal. How exciting! Let’s take a look!
What does their data actually show?
“Following psychosocial assessment at the GIDS, on average 38%–40% of all clients attend the joint endocrine clinics, although this varies across the age range.”
That seems a clear statistic. It appears that 38% of children go to endocrine. It is strange that they have chosen to provide an average percentage across all age ranges, when they are only taking data over a 4-7 year time window. They acknowledge, straight up, that the 38% figure is an underestimate as the older cohort (who are more numerous) proceed to adult services for endocrinology. They do not however, acknowledge that the youngest cohort are too young to be eligible for endocrinology making the 38% figure even more of an underestimate. It is strange then for them to have chosen to lead with this largely meaningless average percentage number.
GIDS do not provide all the data, but do provide a graph which will assist with testing this 38% figure.
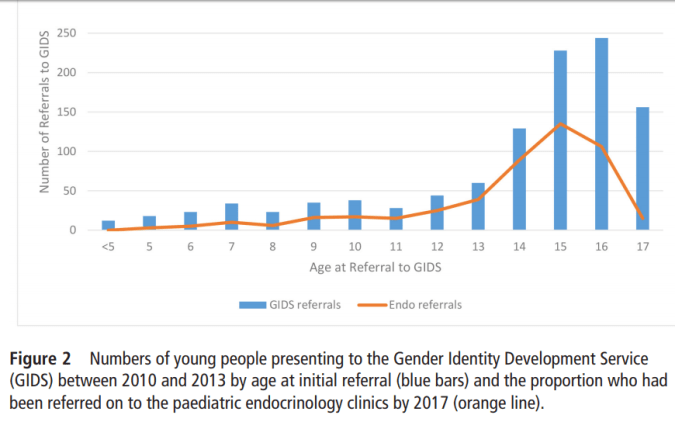
The blue bars track the age at initial referral. The mean age of referral to GIDS was age 14.4 years (the mode would be a more useful statistic in this graph).
The orange line tracks the proportion who had been referred to endocrinology by 2017.
While the underpinning evidence is unfortunately missing, we can use the data visually presented in the graph in order to test the accuracy of the 38% figure for different age groups.
In the graph we are given a single combined data set for the period 2010-2013. For the sake of a simple calculation, we’ll take a single yaer within this (2012) and assume that everyone has been referred in 2012 (rather than 2010-2013 – taking the latter of the mode numbers, as referrals have risen each year).
4 year olds (age of referral) in this data set
4 year olds referred in 2012 are 9 years old in 2017. Unsurprisingly zero out of approximately 10 of these children have been referred by 2017 (they are too young to be at tanner stage two, especially as those children referred at age 4 were more likely to be assigned males who typically start puberty later than assigned females).
6 year olds in this data set
For 6 years olds referred in 2012, who are age 11 in 2017, roughly 3 out of 20 have been referred to endocrinology. Again, this is not surprising. The majority of referrals at 6 are assigned males and most assigned males have not started tanner 2 at age 11.
9 year olds in this data set
For 9 year olds in 2012, who are 14 years old in 2017, we can see around 50% have been referred (20 out of 40 children).
12 year olds in this data set
Children referred at age 12 are age 17 in 2017, and we can estimate about 80% of them have had a referral. Similar for those referred at 13 and 14 years old,
15 year olds in this data set
For children referred at 15 years old, 50% have had a referral to endocrinology a drop compared to 14 year olds at referral.
For 16 and 17 year olds the referral rate drops further. As GIDS explains in their paper, many 15, 16, 17 year olds will have limited benefit from blockers, and many prefer to wait until adult services (transfer at 17) where they are allowed to go on to HRT without the children’s service mandatory year on just blockers.
Some assigned females presenting to gender services at age 16 choose to go on the pill through GP rather than blockers through GIDs and go direct to adult services as they know those being referred at 16 will not get referred for Testosterone in the children’s services. Adolescents presenting in late puberty have less benefit from blockers and service users reports indicate a greater reluctance of GIDs to prescribe for those entering the service at ages 15-17.
Wait just one moment here!
Let’s look again at exactly what head of service Polly Carmichael, co-author of this paper, said on national media on the 7th July 2017 [10:20 am]:
When asked by the presenter Victoria Derbyshire
“How often might you see a child at a young age, 3 or 4 or 5 who as they grow or mature eventually change their mind?”
Polly responded:
“Those that are referred to the service at 5 years old it will only be 6% of those who ultimately go on to seek physical interventions to change their body”
We are now able to check Dr Carmichael’s statement against this newly published data:
For 5 year olds referred in 2010-2013, we are not given the number who have received referral to endocrinology by 2017, but from looking at this graph it is a very low number, it may well be as low as the 6% stated by Dr Carmichael. What does this 6% mean? Let’s dig deeper into this exact issue, using both the above graph and GIDS own referral statistics from their website:
| Year |
Number of 5 year olds referred |
Age in 2017
|
| 2010 |
3 |
12 |
| 2011 |
3 |
11 |
| 2012 |
8 |
10 |
| 2013 |
10 |
9 |
|
| Total: |
24 |
| Average age: |
9.95 |
The entire data set for 5 year olds is 24 children. The average age of their sample in 2017 is age 9.95 years old.
If we were to make the assumption that 100% of these children would wish to access puberty blockers, how many of those 9.95 year olds would reasonably be expected to have accessed puberty blockers in 2017?
GIDs own figures suggest younger children (including 5 year olds) are by far more likely to be assigned males – with 4 times as many assigned males as assigned females at this age.
What then, is a common age for assigned males to start puberty? This 1980 publication states that puberty for assigned males begins at age ranges 9.7 to 14.1 years.
We would therefore expect a very small number of our 24 children to have started puberty. So we would expect a very small number of our children to have reached the stage of being eligible for puberty blockers. The figure of 6% having been referred to endocrinology after the start of puberty sounds a reasonable figure given most will not yet have reached tanner stage 2 of puberty.
This data TELLS US NOTHING about how many 5 year olds referred in 2010-2013 will end up needing medical interventions.
This data DOES NOT justify the Head of GIDS going on national television and, in response to a question on whether young children ‘change their minds’ answering that ‘only 6%’ of 5 year old continue. It is dismissive and damaging.
This dismissive and damaging rhetoric from GIDS directly feeds into (and is a contributor to) the moral panic that we are facing in the UK today around trans children.
This dismissal and erasure of trans children feeds into the situation in the UK where transphobic groups hold meetings stating on camera ‘trans children do not exist’. Where transphobic groups write damaging schools guidance that has been compared to conversion therapy.
GIDS and their anti-fact media messaging is complicit in the harm that is being caused to trans children across the UK.
Misleading manipulation of data
A person who reads this article quickly, glancing at the headline statistic and taking a cursory look at the graph will likely take away two things 1) that only 38% of children go on to endocrine treatment, and 2) that those most likely to go on to endocrine are those referred at age 15 (due to the authors decision to present a graph appearing to show a peak at age 15). These two conclusions would both be wrong. GIDS either lack basic competence at data communication, or are actively intending to misrepresent the data.
On a similar note, they are using their Fig 2 graph to discuss the percentage of children who have been referred to endocrinology. Why then are they showing us a bar chart of numbers entering the service and a line graph of numbers referred, and expecting the reader to guess the percentage. It would be far easier to simply provide a graph of the percentages. The apparent hump on their graph at age 15, fits their mantra that ‘almost all trans children desist at puberty’, whereas a graph showing percentages would have a peak at about age 11. This is manipulation of data to fit a misleading narrative.
‘Desistance’ during early puberty
Head of service Polly Carmichael has talked about the Dutch ‘evidence’ that nearly all trans children will change their mind and not go down a medical intervention path. This ‘evidence’ has been shown to be false multiple times and is now even rejected by the Dutch authors themselves who claim to have been wrongly interpreted. Polly Carmichael claims that GIDS’ own data corroborates the (now withdrawn) findings of the Dutch. She describes a ‘paradox’ that the vast majority of trans children stop being trans at puberty, whereas the vast majority of children referred after puberty do continue being trans. She has a ‘hypothesis’ that early puberty natal hormones are responsible for a change of heart in those referred pre puberty. On the basis of this ‘hypothesis’, the hypothesis that the majority of trans children ‘desist’ during early natal puberty, GIDS delays provision of hormones blockers, and tells service users that prompt provision of hormone blockers may ‘change the outcome’ and solidify a trans outcome.
We can now test this hypothesis using this new GIDS data. How can we test it? We focus on children who were referred before the start of puberty, selecting the older pre-pubescents for maximum age at time of sampling. We therefore focus on children referred at age 9. The majority of 9 year olds have not yet started puberty.
If the GIDS hypothesis is correct, and the vast majority of pre-pubertal children do not go on to medical intervention, we should spot this trend in those referred at age 9. We should see less than 20% of those referred at age 9 going on to referral to endocrinology.
Let’s look at the data. Children aged 9 in 2010 are 16 in 2017. Children aged 9 in 2013 are aged 13 in 2017. Looking at their referrals data, the average age of this group in 2017 is 14.2 What percent of 9 year olds (at referral) in this data set have been referred to endocrinology by 2017? 50%. Fifty percent.
THEIR OWN DATA CONTRADICTS THEIR HYPOTHESIS!
Their own data contradicts their hypothesis that the vast majority of children referred pre-puberty do not go on to endocrinology. Their own data shows that 50% have gone on to endocrinology by the time they are (on average) aged 14.
We know that 50% (20 out of 40 – estimate from looking at graph – actual data is not provided) have had a referral to endocrinology by 2017. Of the other 50% (20) GIDS tell us nothing (despite proposing their percentage as a noteworthy finding). Many questions are left unanswered. How many of those 20 who have not been referred to NHS endocrinology have skipped GIDS gatekeeping and gone to private healthcare services in the UK? How many of those 20 have gone to the USA? We do not know. How many of those not (yet) referred will go on to a referral to endocrinology but have not yet reached tanner stage 2 of puberty (remember, nearly half of this sample are aged 13 or under in 2017). How many are wanting a referral but have not been approved by GIDS, having not yet jumped through the right hoops in their answers or cooperation. How many are denied due to co-existing challenges or circumstances that allows GIDS to deny or delay referral (eg being out of school, being neuro diverse, being too depressed or suicidal, being insufficiently binary, or having a presentation that doesn’t match with GIDS expectation of what a child who is trans will look or act like). How many are wanting a referral but have not had the support of their parents for referral to endocrinology? We must remember that the majority of parents of children at the GIDS are unsupportive, and unsupportive parents can block (and certainly delay) a referral to endocrinology. How many are of these ‘desisters’ are *still trans* but have decided against taking puberty blockers at this point in time due to other life factors, such as exams, travel, other medication. None of this is explored in this paper.
A reflection on data reliability: GIDS data doesn’t appear to be reliable. There is a discrepancy between the total referral figures shown on their website, and their assigned-gender disaggregated figures released through a 2017 Freedom of Information Disclosure. For the year 2012-2013 the former states 3 five year olds (the FOI lists 0 five year olds). For the year 2013-2014 the former states 10 five year olds (the FOI lists 6 five year olds). These discrepancies bring into question GIDS data management.
Pubertal status
On the timing of puberty blockers, GIDS states:
“It is a requirement, according to the Endocrine Society and WPATH guidelines and UK service specifications, that a young person has commenced puberty before any intervention is agreed, as the GD may resolve once puberty commences.
First, Endocrine and WPATH guidelines (SOC7) do of course require puberty to start before prescribing blockers (blockers serve no purpose pre puberty). However, the endocrine society’s position is misrepresented. The Endocrine society says:
“We recommend treating gender-dysphoric/gender-incongruent adolescents who have entered puberty at Tanner Stage 2”.
“At” tanner stage 2. The Australian SOC is even more clear:
“Puberty suppression is most effective in preventing the development of secondary
sexual characteristics when commenced at Tanner stage 2″
“At” Tanner stage 2. The difference between recommending blockers at tanner stage 2 and a requirement that a young person has commenced puberty before any intervention is agreed may sound inconsequential, but this emphasis has profound implications for UK trans children. GIDS have no urgency about prescribing at tanner 2 – indeed they actively encourage delays, believing that a longer period of ‘natal’ puberty is a good thing.
“It is a requirement, according to the Endocrine Society and WPATH guidelines and UK service specifications, that a young person has commenced puberty before any intervention is agreed, as the GD may resolve once puberty commences.
The GIDS statement ‘GD may resolve when puberty starts’ does not appear in either the endocrine guidelines or WPATH (SOC7).
GIDS is fraudulently linking their pet theory (GD resolving when puberty starts) with the more respected evidence from the Endocrine Society / WPATH. This is misrepresentation. No evidence is provided for this claim.
This aligns with Polly Carmichael’s pet theory of natal pubertal hormones making trans children turn cis. A theory she has been speculating about for over a decade. A theory she has never provided a shred of evidence for. Here she is a decade ago saying the same non-evidenced theories she clings to to this day:
“if you halt your own sex hormones so that your brain is not experiencing puberty, are you in some way altering the course of nature?”
A decade ago she was saying the same thing that she says to the media today, that there is not enough long term data on the outcomes of puberty blockers:
“The Dutch data looks promising. But they have not been doing it for so many years that you have long-term follow-up. The data is not over a long enough period of time and that concerns endocrinologists.”
<https://www.theguardian.com/society/2008/aug/14/children.youngpeople>
Her position has not changed in one decade. Her position has not changed because she is not listening to trans people, she is not listening to parents of trans children, and she is ignoring medical experts who disagree with her.
In both psychiatry and social work the term “defensive practice” is used to describe a deliberate practice of risk averse decisions, strict adherence to protocols and lack of learning. Defensive practice is also associated with an organisational culture in which leaders are not challenged (Whittikar & Havard 2016).
This term accurately describes how the GIDS leadership have become stuck in defending their (outdated, pathologising, harmful, non evidence-based) ways of working. They have become defensive, and in defending, have failed to evolve, failed to adapt and failed to remember their primary responsibility – ensuring the best possible outcomes for their clients (trans children and families). Alongside defensive practices they bring an inherent cisnormativity and transphobia – in which their model actively aspires towards and prioritises a cis or ‘not trans’ outcome, above the well being and happiness of their service users.
Persistence
The GIDS paper moves on to talk about persistence (the problematic history of this term, and implication that ‘persistence’ is undesirable, is not explored in the paper):
“Fig 2 demonstrates the low absolute numbers and proportion of prepubertal children with persistent GD.”
FIG 2 DOES NOT SHOW THIS.
Fig 2 shows the percent of children referred to GIDS between 2010 and 2013 who by 2017 had been granted by GIDS a referral to the paediatric endocrine service.
It shows about 80% of those referred at 10 years old are granted a referral to endocrine. For the younger children, those aged 5 in 2012 are only aged 9.95 in 2017 and most of them have not yet started puberty. This study tells us nothing about how many of those 5 year olds will receive a referral to endocrine at some point during their adolescence.
Importantly, this study does not tell us anything about how any of these children identify. It tells us nothing about their dysphoria.
FIG 2 does not tell us the proportion of prepubertal children who have ‘persistent’ Gender Dysphoria. THIS IS FALSE.
By conflating a referral rate with a ‘persistence’ rate, it also equates requirement for endocrine interventions with identity – ignoring the diversity of needs amongst trans children, including those who absolutely ‘persist’ in an identity different to the one presumed at birth, but do not need/choose to take hormone blockers/medical transition.
By conflating a referral rate for persistence, it also overlooks (as far as we can tell from the limited information they publish), those who seek private treatment or pursue treatment overseas.
The data completely ignores the issue of gate-keeping. GIDS are extremely conservative about referrals to endocrinology, and known to discriminate against children with mental health issues, those who are neurodiverse, those who present later, those who are non-binary. We do not know how many of those who have not been referred to endocrine desperately want a referral, but have not yet been granted one.
Finally, we know that two thirds of teens in the service are not supported by their parents. Teens who are unsupported are much less likely to get a referral to endocrinology. How many of those counted as not having been referred to endocrinology have had their referral blocked or delayed by unsupportive parents.
None of these factors are acknowledged in the article.
The article overall conjures up the unsubstantiated claim that ‘GD may resolve’, falsely creates an untrue 38% referral rate (which GIDS themselves clarify in the text is an underestimate of the reality), and mis-describes their referral rate as a ‘persistence’ rate. They use this to dismiss the existence of and undermine the rights of trans children.
Pathologising language continues
The next section provides an overview of the many tests they have carried out on trans children to look for reasons for being trans.
“Endocrine assessment of the reproductive axis of the birth-registered phenotypic male….”
The phrase ‘the birth registered phenotypic male’ is extremely pathologizing and othering language for trans girls. The phrase trans girl, trans feminine people, or people assigned male at birth would be a less offensive replacement.
“A search for sources of hyperandrogenism in adolescent birth-registered phenotypic females in an attempt to explain the dysphoria has not elucidated any differences from a control population”
“It therefore appears that GD is not associated with excess androgen production in postpubertal phenotypic female”
“our search for genetic, endocrine and radiological diagnostic markers of a dysphoria-related state has proven negative”.
How many of these children gave informed and voluntary consent to these unrequested, unwanted, pieces of research, with little relation to their care? Why have UK researchers been focused on a quest to find a diagnostic test for transness, and not on the key challenges, how can we help trans children to have good mental health and wellbeing?
GIDS are so detached from seeing trans children as important individuals with hopes and dreams and high potential. They fail our trans children time and time again.
Fertility preservation
“Various medical options are considered in case of a desire to revert to their birth gender in subsequent years after irreversible treatments have occurred, or in case assisted conception techniques might be called on in adult life to assist with starting a family”
This paragraph is strange. There is no information here. No evidence on what they are talking about re ‘revertion’ after irreversible treatment. No information on numbers.
Talking about a desire to revert after irreversible treatment is a subject that needs handling sensitively with careful context. Everyone working in this field is aware that a tiny number of examples of adults with ‘regret’ are used by anti trans lobbyists to undermine and deny care to trans children.
This report is not however, by anti trans lobbyists, but advice to non-specialists focused on working with children.
Partially irreversible treatment in the form of cross sex hormones is only available from around age 16, and GIDS only permits the children with the most straight forward diagnosis and a long history of gender dysphoria, who have already been on blockers for at least a year, to access HRT at age 16. The gatekeeping is extensive. How many children can they really have seen in the youth service who have had a clear enough history and presentation to receive blockers before 15 and HRT at 16, have had HRT long enough for irreversible changes, and have sought to reverse changes by age 17 before leaving children’s services. Knowing their conservative interpretation of the protocols, I do not believe this has happened in any significant numbers, certainly no evidence is presented in this paper or any other publications from GIDS that I am aware of.
If they are talking about data on regret from other services – they need to be providing a published reference for this statement. The fact that they do not provide a reference, suggests to a reader that they are talking from their own experience. They are scaremongering without providing any data.
Blockers
“In those whose GD is clearly established and long-standing and who have participated fully in the multidisciplinary assessment process at the GIDS, GnRHa is the recommended first-stage medical intervention”.
This shows how conservative they are at offering blockers. Adolescents need ‘established and long standing’ GD. These are subjective quantities. How many months or years is enough? How does an adolescent prove this? It seems like only the most straight forward (insistent, consistent, persistent, though they avoid these terms) are eligible. Yet blockers are intended to provide thinking time for those who are distressed about puberty and need thinking time to explore their identity. Children with the longest history and clearest presentation arguably do not have any reason to go onto (just) blockers, with practitioners in the US increasingly bypassing blockers to go straight to HRT for the simplest cases. It is those children who are less sure, who are questioning, who started to question (or vocalise) their gender at the onset of puberty, who need time to think and would most benefit from blockers. This is the very group who are ineligible.
Note also the requirement to have ‘FULLY participated in the multi-disciplinary assessment process’. There is a vast and unacknowledged power dynamic here. This evidences how GIDS wield their power and absolute authority. Adolescents and families are afraid to advocate for their rights, afraid to challenge clinicians who ask inappropriate questions, afraid to not complete pathologising questionnaires that themselves induce dysphoria and have subsequent negative impacts on the mental health of adolescents. There is no service user autonomy. The powerlessness of children and families adds to stress and feelings of having no control over the future – a powerlessness that greatly harms the mental health of trans and gender questioning children and adolescents.
“The fact that between 73% and 88% of children attending gender identity clinics who present prepubertally, whether they have socially transitioned or not, are likely not to continue with their intention of changing their gender once puberty has started”.
They are listing the 2008 Wallien and Cohen-Kettenis study as their reference. We have discussed this at length in a previous blog.
Even if we just accept their data and overlook the methodological flaws in the Wallien and Cohen-Kettenis study, from the children initially classified as GD who were later re-assessed, 21/36 were ‘persisters’ and 15/36 were ‘desisters’. So even the data in this study shows a 58% persistence rate not the 27% rate that GIDS have quoted using this very reference.
Those who have been paying attention to the current discourse, will be aware that several articles have been recently published criticising the desistance rate myth (the myth that such enormous percentages of children desist from a trans identity). Ehrensaft published on this topic months before this paper came out (notably omitted from GIDS’s references). Since GIDS’ paper was in print, there have been three consecutive publications by a team including Kelley Winters, making clear that these high desistance statistics are simply false. Steensma and Cohen-Kettenis, the latter, one of the authors of the paper GIDS quotes, have also published a new article stating that their work has been misrepresented and does not support high desistance rates.
Here’s Steensma and Cohen-Kettenis in their recent paper (2018):
“The classification of GD [Gender Dysphoria] in the Wallien and Cohen-Kettenis (2008) was indeed based on diagnostic criteria prior to DSM-5, with the possibility that some children were only gender variant in behaviour. We have clearly described the characteristics of the included children (clinically referred and fulfilling childhood DSM criteria) and did not draw conclusions beyond this group, as has wrongly been done by others”.
Cohen-kettenis is here, the very author of the paper that GIDS quotes, stating clearly that others have been wrongly misrepresenting her own work (she is one of the two co-authors of the 2008 Wallien and Cohen-Kettenis study). Cohen-kettenis here, provides final clarity that her 2008 study includes children who are not trans and merely non-conforming.
Yet GIDS have taken this study and wrongly interpret as “The fact that between 73% and 88% of children attending gender identity clinics who present prepubertally, whether they have socially transitioned or not, are likely not to continue with their intention of changing their gender once puberty has started”
The study they use as the reference included children who were just non-conforming and not trans. It did not consider which children were socially transitioned. And it most certainly does not say that children who have socially transitioned (a group much less likely to include children who are just non-conforming ) have the same ‘persistence’ rates as children who have not socially transitioned.
Butler, De Graaf, Wren and Carmichael HAVE FABRICATED THE STATEMENT ‘whether they have socially transitioned or not’.
They have not provided a single reference for this claim.
This is unprofessional, unethical and OUTRAGEOUS.
The ‘desistance’ myth (the myth that the majority of trans children become cis at puberty) has been propagated by Zucker and by the Dutch school, which includes Steensma and Cohen-Kettenis. The Dutch have now publicly distancing themselves from association with this myth, claiming to have been misunderstood and misquoted. Zucker clings to this myth, but is now disregarded as totally out of touch with modern evidence based practice.
GIDS, meanwhile, are clinging desperately to this myth. They need this myth to justify their pathologizing and cisgenderist approaches. If they acknowledge that they are badly mistaken on the assumption that trans children end up cis at puberty, they would have to start asking what else they have got wrong.
The leadership at GIDS, the authors of this paper, are not capable of this mental step – if they acknowledge how badly they have got this wrong they would also have to acknowledge the harm they have caused their whole career.
“Some may ‘desist’ completely, with their initially perceived dysphoric feelings pointing towards developing homosexuality”.
This statement is drawn from the thoroughly discredited ‘desistance’ literature. Furthermore, there is a lot of confusion (and hysteria) in the UK media about the difference between gender identity and sexual orientation. Credible clinicians would in this section state that transgender individuals have a variety of sexual orientations and that gender identity and sexuality are different things.
“GnRHa is prescribed in standard doses for a minimum of a year before additional medical interventions can be considered”.
This requirement to have a minimum one year on blockers, regardless of age or stage of puberty, is not supported by WPATH SOC 7, nor by the Endocrine Society, nor is it in the NHS Service Specification which GIDS are committed to work within. Parents who have complained of the health impacts of forcing 17 year olds to spend a year on just blockers before HRT are reassured that minimum one year is not an official policy. Yet here it is again in writing. This one year minimum on blockers without HRT for late puberty adolescents is not evidence based and is not an approach followed in other countries – not even in neighbouring Scotland. GIDS are here applying a rigid protocol, against their own service specification, unsupported by evidence. 18 year olds in adult services would not be required to have any time on blockers before HRT. 17 and a half year olds in GIDS are forced to have a year on just blockers, regardless of side effects, regardless of not wanting to take blockers.
GIDS uses their monopoly to wield absolute power over trans children and adolescents.
Psychological benefits of GnRHa treatment
“Most young people welcome the ‘blocker’ intervention as helping them to feel more comfortable in their bodies while holding future gender options open. However, our psychometric data suggest that although it permits further time for exploration, the impact on reducing psychological difficulties is limited. Further research is needed to determine whether GnRHa treatment is beneficial for young people of all ages, or whether some age groups may benefit more from this particular treatment than others, perhaps younger rather than older adolescents?”
The evidence is clear that medical intervention for distressed trans youth is the best way of securing improved mental health. It is not surprising that blockers alone do not provide an improvement – HRT (or surgery) are the treatments that distressed trans youth (trans youth who seek a medical transition) need – blockers are simply a delaying method, to ‘buy time’. While they mitigate the fear of future changes, blockers are not in themselves a treatment which treats dysphoria. They simply delay a decision.
Eligibility for cross-sex hormone/gender-affirming hormone treatment
“Cross-sex hormone treatment, currently referred to as gender-affirming hormone treatment (namely the induction of the opposite-biological sex puberty using testosterone in a phenotypic female and oestradiol in a phenotypic male)”
There is a reason why the term ‘gender affirming’ hormone treatment is used. There is a reason why ‘opposite biological sex puberty in a phenotopic female’ is not used. Stop pathologizing trans people!
“(HRT) may be considered once full commitment to the preferred gender has been confirmed”
It is not a ‘preferred’ gender. My child would ‘prefer’ to have her gender match her assigned sex.
“At the GIDS there are psychosocial criteria that need to be met, including that the young person shows some evidence of presenting coherently in the gender role with which they identify and that mental health difficulties are not escalating.
Coherent gender role! This sounds like some 1950s housewife stereotyping. It is 2018 GIDS!
“At the GIDS there are psychosocial criteria that need to be met, including that the young person shows some evidence of presenting coherently in the gender role with which they identify and that mental health difficulties are not escalating.”
Trans youth have to demonstrate distress to be eligible for HRT. But not too much distress. Just exactly the right amount of distress.
“The capacity to give informed consent is an absolute requirement prior to commencing sex hormone treatment… It is acknowledged by the Endocrine Society that a young person under the age of 16 may not have sufficient psychological maturity to commit to such a lifelong and life-changing decision”.
Here’s what the Endocrine Society actually says:
“Clinicians may add gender-affirming hormones after a multidisciplinary team has confirmed the persistence of gender dysphoria/gender incongruence and sufficient mental capacity to give informed consent to this partially irreversible treatment. Most adolescents have this capacity by age 16 years old.”
The Endocrine Society states that most adolescents have maturity by the age of 16. GIDS changes this to “the Endocrine Society” says “under 16s may not have sufficient psychological maturity to commit to such a lifelong and life-changing decision”. GIDS has changed the emphasis and padded with additional spin. This introduces a focus on “life-changing” that is not in the Endocrine guidance. This is misleading.
The GIDS paper attributes to the Endocrine Society and to WPATH SOC 7 the statement:
“no evidence is available to understand the effects of giving gender-affirming hormone treatment before 16 years”
They do not include any reference to a key part of the Endocrine Society’s guidance:
“We recognize that there may be compelling reasons to initiate sex hormone treatment prior to age 16 years”
And they have misconstrued what the Endocrine Society has actually said which is:
“there is minimal published experience treating prior to 13.5 to 14 years of age”
GIDS have completely changed the Endocrine Society’s position on age of eligibility for sex hormones and have claimed the Endocrine Society says there is no evidence for under 16s, when in fact the Endocrine Society says there is no evidence under 14.
Further the GIDS paper fails to mention that the WPATH SOC7 states:
“Adolescents may be eligible to begin feminizing/masculinizing hormone therapy, preferably with parental consent. In many countries, 16-year-olds are legal adults for medical decision-making and do not require parental consent”
“Refusing timely medical interventions for adolescents might prolong gender dysphoria”
“withholding puberty suppression and subsequent feminizing or masculinizing hormone therapy is not a neutral option for adolescents”
Gender affirming hormones and height
“The dose increase schedule is conducted more slowly in those who have never completed puberty in their birth sex to allow emotional and social maturation, as well as the completion of the adolescent growth spurt in height”.
Some trans girls are dysphoric about their height and fear further height will make their lives harder. They are nevertheless kept on a low HRT dose, and keep gaining height, without being told that an increase to their HRT dose could stop further height.
Over 90% go to adult services
“over 90% of those attending endocrinology clinics request further support from adult gender identity clinics”.
Surgery for adults
It is questionable why there is any discussion of surgery in a paper which is focused on children and adolescents, who are, by definition, ineligible for surgical interventions. A critical reflection leads to a conclusion this is included simply to provide further opportunity for scare mongering.
“Male-to-female feminising genitoplasty is a well-established procedure where the penoscrotal skin is refashioned to produce the vagina and labia with preservation of the glans and neurovascular bundle to form a clitoris capable of orgasm. Concern now exists that the early blockade of puberty may result in insufficient genital skin being available for this procedure”.
This statement fails to mention well established alternative surgical techniques being used for those who received early puberty blockers. Puberty blockers have been used since the mid 1990s, and hundreds of young adults around the world who received blockers have gone on to access successful gender confirmation surgeries with extremely high rates of satisfaction and extremely low rates of regret. Stating the concern without mentioning that trans adults who received early puberty blockers have already had successful surgeries, is unnecessary, un-evidenced scaremongering.
“In full male genital reconstruction, a penis can be formed from either abdominal, thigh or forearm skin flaps. A hydraulic implant is inserted in a newly fashioned scrotum to provide controllable erectile function. This approach requires several surgical procedures and leaves extensive scarring”.
The focus on scarring without any mention on levels of satisfaction with surgery, is unhelpful.
There is a brief mention that “the few longitudinal follow-up studies that have been published in the Netherlands have generally shown a high satisfaction outcome, particularly from those who have gone through surgical affirmation of their identified gender. It is useful here to also note a recent Dutch paper from Wiepjes et al (2018)
“6,793 people visited our gender identity clinic from 1972 through 2015 .. Only 0.6% of transwomen and 0.3% of transmen who underwent gonadectomy were identified as experiencing regret” [note the Dutch, like GIDS, offensively use transwoman as a noun]:
Long-term outcomes
“In the UK, as yet there is little evidence of the longitudinal outcome from the GIDS”.
So do some proper research! Focus on topics that will inform clinical decisions. Design research in collaboration with service users and their families. Design research in collaboration with those already undertaking well-funded, large cohort, longitudinal studies in the USA and Canada.
Conclusion
“The UK, along with other developed countries, is seeing an increase in the number of young people who are questioning their gender and taking the decision to pursue social and medical transition in line with their identified gender which may be non-binary. While professionals need to treat young people with respect and to acknowledge the intensity of their gender identification, much is still to be ascertained about the impact of medical intervention. The best practice in this field currently involves close collaborative working in multidisciplinary teams”.
So the key conclusions they want their readers to take away are …. er…No. nope. Nothing clear or useful here.
We need to acknowledge that the vast majority of professionals, raised in a cisnormative and transphobic society, start with negative and sceptical views of trans children. How does this conclusion in any way helping educate and advocate for trans children?
References – hold on, this is interesting
The references are perhaps the worst part.
Some references are core texts that have to be referenced (DSM, Endocrine guidelines, WPATH SOC 7 and the NHS’s service specification)
Several are references from figures with a controversial history of transphobia (eg Blanchard and Zucker).
Most references are from their colleagues in the Netherlands.
There is an interesting article (not referenced by GIDS of course) called ‘Cisgenderism in psychology: pathologising and misgendering children from 1999 to 2008′. It talks of an ‘invisible college’ of gender specialists who often collaborate on joint publications, comprising those who worked most closely with Kenneth Zucker, and who until recently held enormous power over trans children worldwide. This collection of clinicians work was reviewed, and it was found that they held significantly more cisgenderist and pathologizing approaches to trans children than other professionals in this field.
I thought it would be interesting to check how many of the references that GIDS have selected include those clinicians know for cisgenderist and pathologising approaches to trans children.
I excluded the references that are core texts (DSM, Endocrine guidelines, WPATH SOC 7 and the NHS’s service specification)– and excluded those publications that are not about trans or gender diverse children).
| No of references where one of the authors is from the ‘invisible college’ ie Zucker or those who have published with Zucker – those who have cisgenderist and pathologizing tendencies |
10 |
|
| No of other references where one of the authors has worked at GIDS (including self-citations |
2 |
|
| No of references from other people in the Netherlands |
4 |
|
| No of references from other sources |
2. (Both on fertility) |
|
What references are not included
More interesting than what references are included is what references are excluded:
- Almost all publications from experts in the US are excluded from this GIDS article.
- Almost all publications from experts in Canada, Australia, are excluded.
- Almost all publications from clinicians who support affirmative approaches are excluded
GIDS erase through omission any peer reviewed evidence that they instinctively disagree with.
This is not how science and evidence works. The authors completely omit an entire body of evidence from the USA which supports a gender affirmative approach helps trans children. Further, they omit any of the growing consensus of publications which criticise the UK’s delayed transition approach as harmful.
Peer review
The article was “Commissioned; internally peer reviewed”.
It is not clear who internally peer reviewed this paper. It is shocking that this has been accepted for publication. More shocking still is that this poor article is the ‘best practice’ that our children can expect from the heads of the UK children’s gender service.
This week a far better article was published in the Lancet. The Lancet article criticises as harmful many of the practices that are still core to the systematically transphobic UK children’s service. UK clinicians are well advised to learn from this new Lancet publication.
Instead of reading and learning from credible material published by those who are trying to help trans children to thrive, GIDS are choosing to look inward, reading and citing work by discredited members of their ‘invisible college’.
Caught in a defensive practice model, left behind by their international peers who support a gender affirmative model of care, GIDS are in an increasingly desperate state.
It is perhaps not surprising therefore that some GIDS clinicians are emboldened to publicly align themselves to the cause of anti transgender lobbyists who believe that transgender children both do not, and should not exist. A ‘pay to publish’ book with the central premise of denying the very existence of trans children, recently received a glowing endorsement from a serving GIDS clinician. The GIDS library later publicly announced the purchase of the same book via its official twitter account.
This book received a scathing review by the Times Educational Supplement who utterly discredited the “masquerade of a scholarly text”. Review quoted at some length below.
The messages of the book are bold. The first is that “transgender children do not exist”. Having dismissed the perspectives of youth, parents, charities, medicine, social policy and the law as “unproven” and “intellectually incoherent”, it suggests that trans youth are a discursive invention. “Transgenderism”, it contends, reinforces traditional gender binaries, propping up the patriarchy. This framework remains undeveloped and the chapters are inconsistent, offering a hotchpotch of pet clichés that sidestep the evidence-base. Trans youth are variously explained by tribal belonging; restrictive femininity; the distressing human condition; childhood trauma; male transvestites’ sexual desires; and really being gay.
Perhaps hopes were pinned on the highest-profile contributor, whose activism is currently aimed at blocking schools from accepting that children may be transgender. But of 57 sources cited in Stephanie Davies-Arai’s chapter, only seven are peer-reviewed research and these are cherry-picked and distort the wider medical and sociological evidence. Meanwhile, editor Michele Moore’s account of transgender theory leans on dated and inaccurate stereotypes of trans identities that make tiresome reappearances throughout. Nowhere is it acknowledged that many trans people experience binary gender norms as tyrannical, or that many (if not all) trans identities actively queer these binaries.
The second message is that children are “transgendered” by adults and that this is “abusive”. The book constructs an artifice of a society teeming with over-eager parents, whereas research consistently shows that trans youth are often rejected by their families and peers. While claiming that they are motivated by children’s well-being, the authors frequently misuse or ignore recent international studies that unequivocally show both high rates of depression, self-harm and suicide among trans adolescents and the safeguarding effects of gender-affirming support. Indefensibly, the book is almost silent on widely substantiated hate crime against trans youth.
Masquerading as scholarly text, this is epistemological chicanery, with the contributors adopting an already vocal repositioning as the silenced minority. In labelling “transgenderism” abusive, they don’t listen to the supposedly abused; in claiming to challenge “the seemingly unstoppable celebration of transgender ideology”, they present arguments neatly aligned with much recent media coverage. The irony is complete, the consequences no less serious.
In GIDS’ journal paper, Butler, De Graaf, Wren and Carmichael are guilty of many of the same techniques of misinformation, distortion, and cherry-picking literature.
This detailed analysis of the GIDS paper has revealed intentional or incompetent manipulation of data, entirely false claims, misquotations, use of pathologising language, and significant omissions of swathes of recent literature.
GIDS is a failing service stuck in defensive practice.
Our children deserve so much better.