Following a Cass Review recommendation, the NHS has commissioned a pilot (the R22 Project) for trans kids under 10.
Very little information is publicly available on this pilot, with its existence first mentioned here, including an embedded link to the R22 referral form (discussed below).
A project proposal for R22 has now been emailed (not to me) sent in response to an FOI. I have had an opportunity to read this project proposal / outline (R22 Project Quality Improvement Full Proposal). I will present my key takeaways here (I’ll share a public link to the documents if/when I receive one).
Social transition as a risk
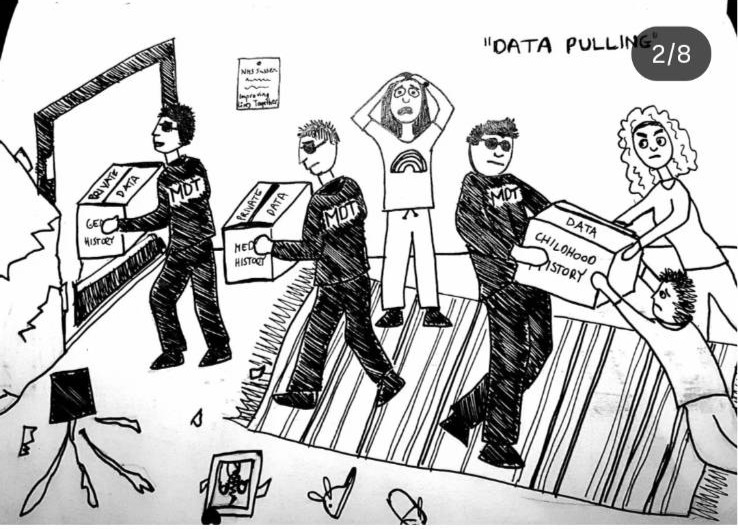
In order to access this pilot, families will be referred to the pilot by their GP. Their GP will fill out a “R22 project referral form”. The form asks whether “safeguarding risks have been identified”, including “safeguarding concerns” and “open to/referral made to children’s social care”. Perhaps noting whether there are any generic safeguarding concern or engagement with social care is active is standard for a GP referral.
Beyond these two boxes, in a section “Any other risks identified” it asks about “bullying or victimisation”. It then asks about “Risk due to social transition (current or future).” Here risk due to social transition is explicitly labelled a risk factor. Of course there is nothing about ‘risk due to family cis-ignorance’, ‘risk due to conversion practices’, ‘risk due to parental transphobia”, ‘Risk due to parental rejection”. Social transition, or even ‘future social transition’ is to be considered a risk.
The pilot has a risk identification section. It talks about a ‘risk’ of equity complaints from families of under tens who are not able to access the pilot. It does not include a risk of complaints from families and advocates related to the harms of the pilot. It completely fails to recognise the highly well established ‘risk’ of the pilot causing significant harm to trans children whose childhood rejection is encouraged and enforced by this ‘support’.
Astonishing levels of knowledge erasure
The project starts from the false Cass Review claim that a majority of trans kids grow out of it in childhood, so long as they are not supported or respected or allowed to socially transition.
The study proposal contains extremely limited references.
Four key references are presented as shaping this project:
1968 Kohlberg Gender Constancy Theory
1981 Gender Schema Theory
1950 Identity Development Theory
1966 Marcia Adolescent Identity
These are all incredibly old references. They are extremely dated pieces of work, written at times where trans children’s identities were not understood in academia. They aren’t even focused on trans kids. They provide nothing of use of trans children.
[I wrote a blog 8 years ago on how bad the NHS was back then on looking to older Zucker literature on ‘gender constancy’ in order to reject the existence of trans kids. I am somewhat shocked to see how much worse they have got in the past 8 years, here focusing on literature from up to 76 years ago].
This is par for the course with the NHS, who continue to rely on really old irrelevant and unethical studies to guide their whole approach to trans children – see here.
Modern psychology research on trans children is completely missing. There is zero reference to work specifically on the same topics refenced above, that actually focused on trans children, including:
2015 Olson, K.; Key, A.; Eaton, N. Gender Cognition in Transgender Children
2018 Gender Development in Transgender Preschool children Olson & Fast
These studies of trans children’s identity development is omitted for purely political reasons. Because it directly contradicts the base assumptions of this whole pilot.
Sample of 12.
One of the key goals for this pilot is to “learn about early presentation of gender non-conformity/distress”.
The one year study, costing over a quarter of a million pounds, aims to target 12 families of children referred to the gender service under the age of 10.
If they are interested in learning about childhood experiences, you might have thought they would at least build from existing literature.
I will note that my own PhD research focused on UK trans children who come out under the age of 10 (a sample who would all have be eligible for this pilot). My own PhD reached 30 such children and families. I had no funding at all for my own research, that was in many ways more ambitious than this current study. Self-funded, and done in my evenings, I reached a sample of 2.5 times what the NHS is aiming for. Unlike the NHS, my study focused on qualitative interviews, actually listening, in detail, to the experiences of trans children and families.
From my PhD I published multiple peer reviewed articles in world-leading journals. These are all on the experiences of trans children who come out as trans under the age of 10:
All of these studies provide meaningful insights into the experiences of trans children under the age of 10, the key goal for this ‘pilot’. They are completely ignored by this project-R22. As are all the other literature on the experiences of trans children under age ten from around the world.
All of this literature is ignored, in favour of really old psychology texts from 1968 because ALL of the modern literature about trans kids provides really clear evidence of the complete wrongness of the NHS approach.
The NHS side-steps this inconvenient truth by sticking its fingers in its ears and pretending modern research with trans children hasn’t happened. It pretends there is a blank slate ready to be filled by this 1-year study of 12 children and families.
Ensuring the NHS gets there quickly
The pilot is explicitly designed so that NHS providers can quickly access the youngest children referred to the gender service. The goal of this quick referral is explicitly to avoid “families seeking advice from non-NHS sources” while on the waiting list, who might “receive guidance that may be discordant with an approach later taken by CYPGS”. The whole goal of the service is to get to families before they hear from other sources i) the huge importance of support childhood social transition (for trans kids who want to be affirmed) ii) the enormous body of research backing up the critical importance of childhood affirmation iii) the body of research backing up the harms of childhood rejection.
“A developmental approach”.
The pilot commits to a ‘developmental approach’ – the NHS’s latest buzzword for non-affirmative and heavily conversive approaches that problematise and reject trans identities.
The service goal is to “safeguard children from narrowing options and opportunities for development of childhood and adolescent identity formation”. The word safeguarding is used by the NHS to remove all opportunities for a depathologised and supported trans childhood.
The document states that “No gender or self-identity outcome is favoured by this approach”. Clearly the NHS thinks this statement is sufficient to guard against accusations of conversion practices. It is contemptible to claim that no outcome is favoured when social transition is explicitly presented as a ‘safeguarding risk’.
This pilot is a continuation of the conversive approach taken by the NHS to trans kids.
Assessment after assessment
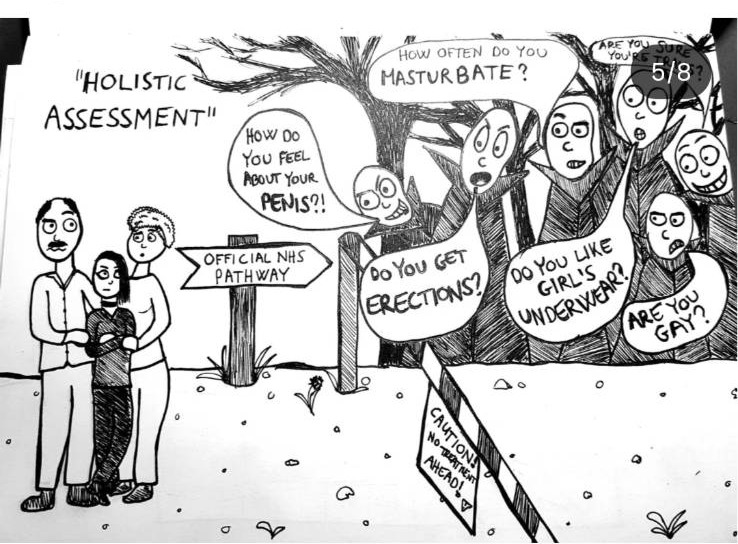
As with everything else in the NHS approach to trans children, the pilot is assessment heavy, with questionnaire after questionnaire. The tools utilised are inappropriate and will be completely ineffective in meaningfully understanding the needs and experiences of this cohort. The assessment is itself deeply problematising. I’ve written about the types of questionnaires used here
Only trans kids?
In the past I would have confidently said that the only kids getting through to the NHS gender service are trans kids, or kids who are seriously considering whether they are trans.
In this new world, I am less confident.
The service cannot even say the word trans. It talks frequently about gender non-conformity.
Will little cis boys be sent to the service just because they like dolls and makeup? Will little cis girls be sent to the service just because they like sport?
Is the NHS taking gender non-conformity back under clinical scrutiny? Are we going back to the 1950s? Who knows.
Adding no value – potentially causing significant harm
The pilot proposes providing ‘education’ to families of trans children. Whilst denying the existence of all modern research. Whilst providing advice that is directly contradicted by all modern research. Let’s be clear – this is not education – this is miseducation. Disinformation. Propaganda. Training parents to enforce cis norms on trans kids – training (and scaring and threatening) parents to reject their trans kids.
One of my specific articles showed the experience of parents who reject their trans kids. This study showed the significant harms of months or years of childhood rejection, focusing on families who came to eventually, in mid or late pre-adolescence support their trans child.
Other articles of mine (for example) drawn from this same cohort of younger trans kids, showed the life changing positive impact of childhood support. Social transition allows trans kids to have a happy childhood. A summary of the literature on childhood social transition showed significant evidence of benefits, and zero evidence of harms.
This pilot is designed for the exact opposite. To educate parents to reject their child.
To deny social transition.
To ensure schools do not support social transition at primary school.
To deny trans kids any opportunity of a safe and happy childhood.
Anti-trans groups love Conversion practices. They have heavily lobbied against bans that cover trans people. They have tried to claim that trans support or affirmative medical care is a conversive practice. They have tried to water down the definition of conversion practices to emphasise only the most physically violent acts. They have tried to bulk up exceptions, based on religious freedoms. They have tried to bulk up exceptions, based on parental rights. They have tried to bulk up exceptions, under the banner of ‘legitimate medical practice’ or ‘legitimate psychological exploration’.
When discussing conversion practices, a lot of the focus is on the idea of a sweeping legislative ban and the details of what is or isn’t criminalised.
In a short blog I want to focus on three aspects of a ban on conversion practices. Here I will focus on:
Part 1: Conversion practices that are designated a CRIME
Part 2: Conversion practices that are widely understood as a BAD PRATICE
Part 3: Removing conversion practices from public HEALTHCARE
I see these as three distinct strands, and it is important to do more that just focus on the first one.
Part one: Conversion practices that are a CRIME
Legislation against conversion practices can be understood as legislation that makes certain practices illegal. It could open up a process for prosecution of abusive practices. It could be legislation used to investigate harmful practice, especially by private practitioners, religious practitioners, parents, where the harm is really huge.
Anti-trans campaigners are working very actively to water down the legislation, to create exceptions, to reduce the chances of conversive practices being deemed a crime.
Effort to tighten the legislation is needed, and I’m sure some folks will focus on that area. For myself, I am perhaps less inspired by the idea of criminalisation as a tool for justice for trans kids – the barriers to actually getting to court are so high, the support is so low. If the more extreme proponents can be actually made to stop practicing under this legislation, that would of course be valuable. I fear that those who are most active will be adept in using the right language to evade a ban, to deny their work is conversive, to exploit the loopholes that have been put into law.
The laws at present have so many loopholes, especially when working in a cisnormative society, that I don’t expect conversion therapy AS A CRIME will hugely protect trans children any time soon.
Part two: Conversion practices that are widely understood as a BAD PRATICE
I am more interested in these bans on conversion practices as a societal indicator of what is understood to be BAD PRACTICE.
I am very interested in the ways in which a Conversion Therapy Ban signals to the general society what is and is not acceptable practice.
With this as a goal, I am less interested in the legislation as an enforceable act for punishment and prosecution of CRIME, and more in the legislation as a route to culture change, of signalling across society what is ACCEPTABLE PRACTICE.
I would prefer to see a really broad legislation that conveys clearly a cultural message – “trans identities are fine and non-pathological” – “efforts to change, repress or suppress trans identities are harmful”. I would feel even better about the legislation if it also mirrored the words of the UN expert of SOGI who explicitly stated that ‘efforts to delay or deny transition’ are a conversive practice.
I’d also love to have recognition, within any work on conversion practices, of a reality that modern conversive practices, especially in psychology or healthcare, know enough to avoid describing themselves as ‘seeking’ to change or suppress identity. They often don’t even think of their work in these terms themselves – instead rejecting the existence of trans identities or presuming that a trans identity is a false misunderstanding. They usually work by compelling or coercing trans people to ‘explore’ their identity, in a manner that is never pushed onto cis people. Conversive practices in psychology or healthcare are less defined by ‘I will do X, Y or Z to make you cis’, and more by ‘we won’t just accept and support your trans identity, we need to first make you do X, Y or Z’.
Within legislation banning conversive practices, broad statements of the practices that are illegal are valuable not only for defining who can be prosecuted for committing a crime. They are equally powerful in setting a clear statement across our societies, that conversion practices are wrong, harmful, and should be avoided.
Part three: Removing conversion practices from public HEALTHCARE
In the UK we have a peculiar situation, of a Government claiming to want a conversion therapy ban, while the same UK Government has put in place an NHS healthcare service that is actively conversive for under 18s.
When we consider the conversion practices that are an intentional part of our public services, especially in the NHS, we need to take a different approach, and not centre our hopes and our advocacy in a legislative ban.
I don’t think we are ever going to be in a world where our UK Government will bring into law a ban on Conversion Practices, and start by prosecuting itself for its NHS trans children’s healthcare service. This is not a realistic hope for conversion therapy legislation.
What we can try to do includes the following:
Advocate in spaces like in Europe, that Governments currently practicing conversion practices in their public healthcare systems should not be at the table in writing conversion therapy legislation. If they are given any such seat, they will obviously re-write the legislation to exclude their own practices.
Argue strongly that a government cannot bring on to paper legislation against conversion practices, whilst practicing conversion practices in its own healthcare system.
Any ‘conversion therapy ban’ in the UK at this time of State level conversion efforts, would be an absolute joke and mockery. I would strongly argue against the imposition of a ban that runs alongside widespread NHS conversion.
There are some folks who clearly think we can bring in a legislative ban first, and then try to use that ban to argue that our NHS healthcare is conversive. This seems a doomed strategy.
While we have any momentum moving towards a ban on conversion therapy, we should argue that such a ban CANNOT be put into practice whilst giving an exception to the conversion practices in our own NHS. The conversation around wanting a ban, can be used as a tool to pressure the Government and NHS to recognise their own roles in conversion practices.
As stated before, the primary purpose of a ban is not in creating a new CRIME for a tiny minority to be prosecuted under (where many of the more easily prosecutable actions could perhaps be prosecuted under other legislation eg actual bodily harm anyway). The purpose of a ban is in shaping societal understanding of what is ACCEPTABLE PRACTICE.
A ban that comes into place whilst allowing current NHS practices is doing exactly the opposite. It is saying that trans conversion practices actually aren’t a problem, if they come with a white coat – if they come with an NHS rainbow badge.
For me, we should advocate for a ban on conversion practices. We should raise our voices. Create pressure in public and politics.
But this advocacy is primarily to shape public opinion, to shape individual practice and to shape institutional practice.
We cannot ignore the HUGE ELEPHANT in the room of our NHS enforcing conversive practices.
We can advocate for a ban on conversion practices WHILST also stating that any such ban is completely impossible and meaningless until the time when we have removed conversion practices from our national policy.
I don’t see a Government written statutory ban on conversion practices as a tool to remove those practices from our Government designed NHS.
WHO IS CONDUCTING CONVERSION PRACTICES?
For those people who are advocating for the introduction of a ban on conversion practices right now in the UK, whilst the NHS is practicing them – I would like to ask the question: Do you really see a ban on conversion practices as being a tool to change NHS practice? Or is it more that you don’t really care about trans kids.
For me, there are five areas of conversion practices that I am most concerned about, that I see most often here in the UK:
1: Our NHS children’s gender clinics, in ways that align with UK Government policy.
2: Other NHS healthcare professionals who are practicing overt conversion practices, in ways that align with UK Government policy.
3: Parents, conducting conversion practices on their own children, many of whom are acting in ways that align with UK Government policy.
4: UK Schools, conducting conversive practices on children in their care, in ways that align with UK Government policy.
5: Private therapists, conducting very explicitly conversive therapy.
Of these, the only ones who could potentially be impeded by prosecution a conversion therapy ban are number 5 – the private therapists. But these people, who are very committed to conversion therapy – are also very aware of the exceptions and loopholes in the law. They will utilise the loopholes that are being written to protect NHS approaches, they will adapt their own language, they will try to evade prosecution – and they will likely succeed. A law that provides exceptions for ‘legitimate therapy’ will be utilised by private conversion practitioners, especially when they only need to argue that their practice is not so different from (abusive) NHS practice.
Parents will be unlikely to be prosecuted anyway, unless they’ve done something really physically abusive that could have been prosecuted under other child protection laws. Exceptions for current NHS practice create a huge scope for justifying conversive parental practice.
Any legislative ban brought in in the UK right now will not protect the majority of trans kids impacted by conversion practices.
And any legislation written on paper, that is deemed compatible with current UK Government conversive policy, in healthcare and schools, has zero value in shifting the societal understanding of what is and is not ACCEPTABLE PRACTICE.
We should keep talking about conversion practices. How they are harmful.
We should keep pressing for a legislative ban.
We NEED to also continue to push attention to a reality – we cannot have a meaningful ban on conversion practices, whilst it remains Government policy. For more on conversive practices in the NHS, see my recent peer reviewed article:
Those advocating for a (much needed) ban, have a responsibility to put as much energy into calling attention to UK Government policy – they cannot push this elephant to the sidelines.
I’m pleased to see the current resolution from the Council of Europe. I think it remains a useful indicator of what is ACCEPTABLE PRACTICE, even while lobbying from the Evangelical Alliance and Sex Matters have tried to dilute its protections.
Trans children have rights under international and domestic law, and we can be more assertive both in calling attention to rights violations, and in demanding institutions uphold these rights in policy and practice.
This accountability should be more robust in Scotland, who in 2024 brought the UN Convention on the Rights of the Child (UNCRC) properly into domestic law.
When the Scottish Government embedded the UNCRC into Scottish law, it made a commitment to children across Scotland: that child rights matter; that decision-makers will be held accountable for upholding the rights of all children.
When it comes to trans children, that promise has fallen short – trans children are seeing their rights eroded and ignored, in healthcare, education and wider society.
Scottish schools are institutions with a legal duty to uphold trans children’s UNCRC rights, yet we are now seeing Government policy advising schools to segregate, humiliate and harm trans pupils. This approach is incompatible with Scottish UNCRC commitments, severely threatening trans children’s safety, well-being and access to education, and placing schools and educational policy makers in violation of their legal responsibilities.
In healthcare we are seeing trans children’s right to safe and equal access to health eroded by policy across Scotland. Scottish children’s trans healthcare policy is not meeting its legal obligations under the UNCRC.
I call on Scottish MPs and MSPs, the Scottish Children’s Commissioner, and all who care about child welfare, to uphold their UNCRC responsibilities, speaking out on current injustices, protecting and upholding trans children’s rights under international and domestic law.
I call on everyone engaging in working with or shaping policy towards trans children to explicitly recognise their legal obligation to trans children. Under UNCRC there is a legal responsibility to listen to trans children, explicitly and directly, in a meaningful way, where trans children’s voices, experiences and priorities meaningfully shape Scottish policy.
The incorporation of the UNCRC into Scottish law is having consequences across Scotland, shaping the way in which institutional policy is defined and evaluated. Trans children need to be part of this process.
We need to hear two statements significantly more often across Scotland: “what does this mean for trans children in Scotland?” and “is this compliant with our obligations to trans children under the UNCRC?”. The first question explicitly recognises the existence of trans children; the second explicitly recognises their rights under the crc. Both questions can only be responded to through close and trustworthy collaboration with trans children, centring their voices and perspectives, and ensuring such voices and perspectives meaningfully shape policy and practice.
For more on trans children’s rights under the UNCRC, see this peer reviewed article, in the leading International Journal of Child Rights, jointly authored with Dr Ruth Pearce from the University of Glasgow.
These UNCRC rights and obligations are relevant in all countries across the world, apart from in the USA (the only country not to have signed up to the UNCRC).
Across the whole world we need to see Governments, policy makers, and individual institutions, from schools to councils to healthcare bodies, recognise trans children’s rights, uphold trans children’s rights, and be accountable where these rights are violated.
[This is really long and is a live-note taking as I read through from pages 27-100 of the report. I won’t do beyond page 100]
Looking for balance
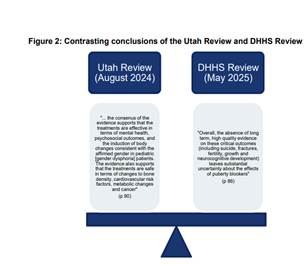
The following image is provided to illustrate contrasting conclusions of different reviews of the same evidence base.
One the left, and in favour of trans healthcare we have the Utah Review:
“”… the consenus of the evidence supports that the treatments are effective in terms of mental health, psychosocial outcomes, and the induction of body changes consistent with the affirmed gender in pediatric [gender dysphoria] patients. The evidence also supports that the treatments are safe in terms of changes to bone density, cardiovascular risk factors, metabolic changes and cancer” (p 90)
On the right, and opposed to trans healthcare we have the DHHS Review:
“Overall, the absence of long term, high quality evidence on these critical outcomes (including suicide, fractures, fertility, growth and neurocognitive development) leaves substantial uncertainty about the effects of puberty blockers” (p 86)”
The graphic suggests that the Vine review is going to have the difficult task of weighing up the benefits vs risks in this field where different reviews come to different conclusions on the same evidence base.
What is unstated, in presenting these two reviews in balance, is the type of evidence they are interested in.
They are asking very different questions. On the left we see some evidence of benefit, for a treatment that is wanted by trans young people, with no evidence of harm. In a rights-based approach, this is convincing.
On the right, we see emphasis of a claimed a lack of rigorous long-term evidence on areas that are assumed to be a risk (suicide, fractures, fertility, growth and neurocognitive development) – without providing evidence that there are a notable or unmanageable risk. We are presented with the claim “uncertainty about the effects of puberty blockers” when the effects of puberty blockers are very well known, with no controversy in cis users.
These two are not of equal status, and presenting them as ‘in balance’ already gives the impression of a review looking for a performance of balance, rather than driven by the actual evidence.
Ignoring the impact of prejudice
There is a box on page 35 that is indicative.
Here the different views are presented:
“The Panel heard in consultation: · diametrically opposed interpretations of, and commentary on, the evidence base underlying the use of PB and GAHT, including criticism from several viewpoints of the methodology and conduct underlying all research; · from some clinicians who highlighted the role of expert opinion in EBM, and others who criticised a situation where opinion replaces evidence, particularly in clinical practices with, or where concerns may be raised of, a closed culture; · concerns of bias in research resulting from low sample size and uncertainty resulting from the lack of longitudinal studies, along with comments regarding the feasibility of studies such as Randomised Placebo Controlled Trials (RCT); and · from some clinicians who highlighted the accepted standards for EBM in current paediatric and psychological medical practice, and others who critiqued the use of these standards.”
All of this is presented without ANY consideration of a very clear reality that this is an area of healthcare significantly impacted by prejudice – where significant actors are fundamentally opposed to trans existence – where actors are proactively trying to shut down all healthcare for trans youth.
Recognition of ‘differing professional opinions’ in this field cannot be separated from the recognition of proactive movements, within healthcare professions, to outrule trans healthcare.
In 2026, in the face of politically and ideologically motivated campaigns against healthcare, from trans healthcare to abortion to vaccination, it is completely unacceptable for an evidence review to pretend that this is not a significant component of what is happening. It is impossible for any healthcare review to try to stay neutral to, much less in denial of the existence of ideological movements trying to eradicate healthcare.
Summary of the evidence
The Vine Review’s summary of the evidence is presented on page 36:
In summary, our conclusions are:
(a) we agree with the near consensus among international reviews (noting the conclusion of the Utah Review),42 that the evidence base underlying use of PB for young persons with gender dysphoria is limited;
(b) the reasons for that limitation include broadly that most studies have methodological limitations, are shorter term, observational only, risk selection bias and risk confounding in that outcomes often cannot be solely attributed to one intervention;
(c) the results of the JBI literature review are set out in further detail below, but in summary, JBI reported a low to moderate certainty trend towards short term psychosocial benefit in care pathways involving PB treatment, however, that effects varied by birth-registered sex, evidence quality is low and some studies reported no change or persisting body dissatisfaction;43
(d) there is no evidence that PB should always be used before starting GAHT;
(e) despite methodological limitations, there exists low quality preliminary evidence suggesting that PB, when used appropriately, can temporarily alleviate existing gender dysphoric distress which could otherwise exacerbate; and
(f) there is some evidence that PB impact bone health in the short to medium term. There is a paucity of evidence as to whether bone health is negatively impacted in the longer term, but bone health should be monitored.
A few thoughts on the above table:
Evidence quality: Amongst all the discussion of evidence quantity and quality (points a and b), there is no recognition of three really important points – 1) that the evidence base is similar to or better than the evidence base for many other areas of medical care 2) that, despite being used and studied for decades, there is no evidence of significant harm 3) that in the absence of any evidence of significant harm, discussions on evidence quality are driven not by medical concern, but by controversy driven by the concerns of those ideologically opposed to all trans healthcare. When we centre evidence base quality without recognising these points, we will set off chasing a phantom – seeking an evidence base that will never be good enough for those who are ideologically opposed to trans healthcare.
Double standards: (On page 37 this double standard is even more clearly stated – the evidence base for use of puberty blockers for precocious puberty is stated thus “when used for central precocious puberty, PB are “generally well tolerated, with no clear evidence of harm to bone health or reproductive function, and uncertain effects on cognition and psychosocial outcomes but further research is required”. Uncertain impacts on cognition and psychosocial outcomes is not a justification for banning healthcare for cis individuals – only for trans healthcare.
Benefits: Here again we see puberty blockers held to an inappropriate evidence base of ‘benefits’. Short term psychosocial benefit is presented as somewhat inconsequential, despite being a key purpose of a puberty blocker. Puberty blockers would never show ‘long-term psychosocial benefit’ because they are not supposed to be used longer-term, and longer-term differences between those accessing or not accessing healthcare would a) be unethical to study in a randomised trial and b) would be confounded by those who also access HRT. The finding of ‘some studies reported no change or persisting body dissatisfaction’ is presented as though a negative, when this is entirely EXPECTED for puberty blockers. Puberty blockers are never expected to resolve existing body dissatisfaction. Why are puberty blockers continually held to inappropriate standards? [Answer, this is intentional, if they are held to appropriate evidence standards they easily pass]
WHOSE VOICE MATTERS? Part d of the conclusions (again, should be obvious) is notable. “there is no evidence that PB should always be used before starting GAHT”. If the review actually centred trans individuals’ healthcare autonomy, it should be obvious that puberty blockers as monotherapy should not be forced onto all trans youth. This is yet another indication that the review is taking an approach to healthcare as though healthcare service users don’t matter. Where is the centring of patient autonomy and decision making? This problem is inherent in healthcare services that try to ‘treat’ the condition of gender dysphoria (centring the view of a clinician on what is the most effective treatment) as opposed to healthcare services providing healthcare to trans communities (centring the views of what trans individuals want/need to access). Of course trans youth who want to access HRT should not be forced onto blocker monotherapy – this conclusion needs to be framed as a conclusion in favour of patient autonomy, not in terms of the evidence base.
WHAT ARE THE HARMS? For a treatment that is strongly desired by trans communities, strongly endorsed as beneficial by trans communities, strongly supported by clinicians who want to deliver that care, any evidence review needs to consider what would be the evidence base for prohibiting it. Especially for a minoritised community facing calls to outrule all healthcare, there is surely a duty on healthcare reviews to establish a bar of necessary harm in order to outrule such care. Here there is no strong evidence of harm from this care. Yet this conclusion – what is the clear (high quality) evidence of harm? There is none, yet this does not make a bullet point. The bias is clear – trans healthcare needs to be continually defended – and those opposed to it do not even need to produce evidence of harm. This mismatch in evidence thresholds is core to all recent anti-trans reviews such as the cass review. Evidence is support of care is never good enough. Concerns about hypothetical harm is taken extremely seriously, no matter how flimsy or non-existent the evidence of harm is.
On page 36 a section of ‘the commission also heard’ a list of important pieces of evidence that are all really meaningful, all of which should guide the review towards individualised trans healthcare.
The Panel heard in consultation:
· from individuals with lived experience and their families, experiences of distress at the prospect, and experience, of developing secondary sex characteristics through natal puberty; · from clinicians and individuals with lived experience, that PB give ‘thinking time’ to young people to explore their gender identity and for their family and clinicians to consider persistence, insistence and consistency and decide whether GAHT is right for them without developing potentially distressing secondary sex characteristics through natal puberty; · from clinicians and individuals with lived experience, that the timing of PB is critical in that they prevent or halt development of secondary sex characteristics but have minimal utility for adolescents presenting to a service at a later developmental stage; · that long waitlists can prevent young people from accessing a PB prescription before their puberty progresses beyond the developmental stage where PB may assist; · that use of PB during early puberty before progression to GAHT results in better passing in the future which is psychologically relieving to young people at the time and in the future, lowers risk of future stigma and discrimination surrounding being identified as transgender and decreases the need for future surgeries such as top and voice surgeries; · from some clinicians, individuals with lived experience and families, that PB prescriptions have assisted school attendance and engagement and psychosocial functioning and experiences of PB assisting with health issues, including suicidality and eating disorders relating to an attempt to prevent pubertal development; · from some clinicians, individuals with lived experience and families, experiences of young people at times feeling socially isolated on PB as they are not progressing through puberty at the same time as their peers and some experiences of psychosocial developmental delays; and · from clinicians, awareness that PB should not be prescribed on a long term basis and that there is a point where the young person must either begin GAHT or cease medication.
The above, combined with no evidence of significant harm, would be highly convincing in favour of any area of healthcare not informed by prejudice.
On this page, in a footnote, the authors also note the way that the Utah Review considered this evidence base: “The Utah Review concluded at page 90-91 that, “the consensus of the evidence supports that the treatments are effective in terms of mental health, psychosocial outcomes, and the induction of body changes consistent with the affirmed gender in paediatric gender dysphoria patients. The evidence also supports that the treatments are safe in terms of changes to bone density, cardiovascular risk factors, metabolic changes and cancer. … it is our expert opinion that policies to prevent access to and use of GAHT for treatment of gender dysphoria in paediatric patients cannot be justified based on the quantity or quality of medical science findings or concerns about potential regret in the future, and that high-quality guidelines are available to guide qualified providers in treating paediatric patients who meet diagnostic criteria”.
The Vine Review should have been more transparent in answering the real question it was tasked with: “Is there medical evidence to justify the denial of this area of healthcare”. The Utah review was honest about having this as its key task, and answered it clearly “it is our expert opinion that policies to prevent access to and use of GAHT for treatment of gender dysphoria in paediatric patients cannot be justified based on the quantity or quality of medical science findings”.
Service user involvement
On p.39 the vine review notes an important criticism of current literature: “no studies reported patient or stakeholder involvement in design or conduct which highlights a critical gap in the relevance and applicability of the evidence”. It is erm interesting, that they disregarded qualitative literature here, a place where patient voice can be found. It is also clear that the Vine review has not considered the incompatibility of trying to centre patient priorities, and achieving an evidence base that will satisfy critic. The two are highly incompatible, and this needs to be recognised. Critics will continually ask for more assessment, more domains of measurement, longer term follow up, and a focus on the treatment of a psychiatric diagnosis of gender dysphoria. Service users will demand rights respecting healthcare that is not subject to excessive and harmful assessment, the right not to ensure life time study, and the need to centre the outcomes that matter to trans young people, not impacts on a deeply dated and flawed diagnosis of gender dysphoria.
Effectiveness of the treatment
Associated with the Vine Review is a literature review from Joanna Briggs Institute at the University of Adelaide (JBI). The conclusion of this literature review as stated on p.39 of the Vine Review is “that no generally positive benefit-risk assessment of PB for the treatment of gender dysphoria of young people can be made on the evidence”.
Their core basis for this statement is “although the evidence for short term benefit in psychosocial areas may be trending towards positive. Evidence for cognitive, bone, fertility, and long term physical health outcomes remains inconclusive or inconsistent, with limited data to assess risks or sustained effects.”
The very next section goes on to say “Effectiveness in suppressing puberty 121. PB are the most effective treatment for suppression of puberty, with no other agents having been shown to be efficacious in this setting”.
The evidence review is always rigged to show ‘no evidence of impact’ whilst also showing ‘PBs are very effective at suppressing puberty’. If patient autonomy was respected, the fact a particular individual ‘wants to avoid incongruous puberty’ would be centred as the treatment goal, and there would be no question of the ‘effectiveness’ of puberty blockers. It is only because we are in this quagmire of determining ‘effectiveness in treating gender dysphoria’ that we are forever being asked for evidence of effectiveness, for a treatment that is very clearly and uncontrovertibly effective at its key purpose (preventing an unwanted puberty).
Again, no consideration of harms of denying care
I am so tired of this type of evidence review. They state (p,41) that “on psychosocial outcomes indicated improvements in depressive symptoms, anxiety, suicidality and quality of life”. They caution that “certainty and causality are low due to the methodological limitations of the research”. Why would you ban a treatment, with no evidence of harm, with this type of indicated benefits, simply due to “methodological limitations of the research”. It is bad faith all the way down.
The answer to this is not to improve the methodological quality of the evidence base, it is to rigorously recognise and challenge the forces that are using questions of methodological quality to try and cancel a treatment that they are ideologically opposed to. Those raising concerns need to be told to come back with rigorous evidence of harm or to go away. I am so tired.
Another double standard
Another double standard appears on p.45. When assessing the benefits of PB, evidence of the positive impact on mental health when combined with HRT is apparently not eligible for consideration when evaluating puberty blockers. But, when considering the risks of puberty blockers for fertility, the assumed addition of HRT is included in the evaluation of risks.
Value of autonomy Page 45 includes important input from those with lived experience on “the value of autonomy in a decision of whether to accept risks of a course of treatment based on the relative importance of the possible risks, benefits and unknowns to them”. This important conclusion is not emphasised in Vine review reflections.
Even those adults whose cared more about fertility as they got older, said that they would not retrospectively change their decision to pursue affirmative medical care “due to the beneficial outcomes they experienced”.
There are some parts of this report that are well written, have good content, particularly the ‘in consultation’ boxes. It feels different to the Cass Review, that was rotten throughout. It smells like a report that started out good, drew upon solid work by more junior folks, and was tweaked and made worse at a top level for political fit (purely my speculation). In the Cass Review it seemed as though every section was authored by those ideologically against trans healthcare. Here the picture is much more mixed.
Failing to centre individualised rationales for healthcare.
P.46 “A rationale for PB use is to improve longer term societal acceptance in the individual’s gender identity”. The reasons for using puberty blockers are presented as though trans youth are a uniform group. There is not enough recognition that every individual is different, may have different priorities, and may want to make a risk benefit analysis of their options differently, shaped by their different priorities and concerns. The need to make an all encompassing ‘rationale’ for puberty blockers stems from the assumption that this is a ‘treatment’ of a ‘condition’, rather than a part of bodily autonomy for a marginalised group. Once you centre bodily autonomy, it is obvious that individuals will have different priorities and different ways of viewing the purpose of puberty blockers or HRT. If you centre individualised healthcare decision making, evidence also moves from a binary is there good enough evidence to allow this or should be ban it (the territory of the Vine Review), to asking what evidence do trans young people need to make individualised informed decisions, and how can we better support informed decision making.
Evidence double standards again
P.47 In one section there is a claim of insufficient evidence of reversibility when PB are stopped without HRT. This is clearly nonsense squared. They don’t even put this into scientific terms. What are they saying is not reversible? Are they saying hormone levels of endogenous hormones don’t increase? Are they saying something else? It is all very vague and unscientific here. If there is a specific concern about some irreversible impact, they need to evidence it – this type of completely unevidenced speculation, that happens to align with anti-trans scaremongering, shouldn’t appear in a report that claims to hold itself to high quality evidence. Another double standard in the very high quality evidence needed to support care, and the flimsy or non-existent evidence that is counted when undermining it.
Burden of proof
In the next box they state “opposing interpretations of whether PB are reversible when used for paediatric gender dysphoria”. But is there any evidence of it not being reversible? What specific areas of non-reversibility have been proved (even anecdotally). Why is there absolutely no minimum standard of evidence for which to critique this healthcare? When making a specific claim (it is not reversible), for a healthcare that has been used for decades, the burden of proof should be on those who are raising this concern to demonstrate that it is not reversible. The burden of proof shouldn’t always be supporters of affirmative healthcare, to prove that a totally unsubstantiated ‘concern’ is not true.
If we allow any unsubstantiated concern to be taken seriously (again, in healthcare used for decades, where that concern is not considered important in cis people), and if we require the affirmative side to produce high quality evidence that this made-up concern is NOT true, then we set ourselves up for continual failure. Trans healthcare can continually be kept under accusation of ‘not proven’, because the goal posts can continually be shifted to new domains of made-up concern. We have already seen this happen over the past decade.
In medicine perhaps there is a tendency to see ‘no smoke without fire’. To investigate rigorously whenever people raise concerns about unintended impacts. But we need to recognise the world we live in – a world shaped by transphobic prejudice. Anti-trans actors will always raise concerns about impacts. There needs to be a burden of proof on those raising concerns to specify and justify their concerns. In trans healthcare, nevermind justify and evidence, they often don’t even specify their concerns. We have concerns over ‘impact on psycho-sexual development’ without even stating what those concern actually are. Here we have concerns over reversibility, without even specifying what irreversible impact they are claiming may occur.
P, 47 has a pretty clear and strong conclusion: “In summary, it appears from the available research that the effects of PB are reversible. They are best started early in puberty and for a limited time. Unwanted side effects are rare, provided there is regular monitoring of relevant hormone levels. If used later in puberty, there may be more side effects, and it may be more appropriate to consider other treatments to address the symptoms or issues which are causing concern, such as menstruation… Having considered the JBI literature review, previous reviews and studies and available guidelines, we have concluded that, with proper oversight and appropriate reporting, there can be benefit for a young person in being able to access PB.”.
It then moves into the unevidenced: “We support treatment only being considered after assessment by a MDT with experience and expertise in this area and only after any other causes or contributors to the young person’s distress have been considered and resolved to the extent possible”. This latter part is entirely unsubstantiated by the preceding evidence review. Apparently evidence must be rigorous when considering a treatment, but strong requirement can be added with zero evidence when this infringes on trans youth healthcare rights.
Why does this very clear statement on the overall support for puberty blockers not make it into the Vine Report Summary of Recommendations or executive summary? Earlier sections of the report focuses only on the limitations of the evidence, not on this recommendation in support of the care.
Here I’ll stop this part of my reading of Vine, having got to p.48.
On HRT
On HRT it notes (p.50) “Overall, the evidence suggests that the treatments induce the desired physical changes and that there is increasing evidence suggesting positive psychosocial outcomes. The evidence also suggests that, in healthy people, apart from the impact on fertility, the risks to bone health and of cancer and cardiovascular events are low and comparable to those in cisgender counterparts.”
Again, did I miss where that is stated so clearly in the exec summary and recommendations? Those bits very much focused on risk, what is unknown.
On HRT effectiveness
The Utah review is quoted in HRT being “effective in terms of the induction of body changes consistent with the affirmed gender in paediatric gender dysphoria patients”.
Why does HRT here get to be evaluated in the terms in which it is used by trans people (to induce affirmative bodily changes) yet puberty blockers aren’t evaluated in the terms by which they are used by trans people (preventing unwanted pubertal changes). Evaluating effectiveness is far more reliable when they are assessed to the purpose that makes sense for healthcare users (preventing non-affirmative or enabling affirmative bodily changes) than in treating an ill-suited diagnosis (gender dysphoria).
Surely this could be considered a basic requirement for evaluation of medical care – evaluate according to the purpose/desired impact of that medical intervention as defined by those taking it.
Trans healthcare goes astray because there is too often no correspondence between the reasons why trans people seek trans healthcare and the ‘treatment goal’ defined by cis clinicians.
False middle-ground
I really disliked the part on page 57 where the Vine review notices polarisation and tries for a middle path “adopting a practical lens that does not engage with these extremes”. There is no recognition that one of the extremes, those fundamentally opposed to trans existence, needs to be isolated and ignored. And that there is no such group at the other extreme – indeed, the suggestion that those fighting for rights-centred healthcare should not be positioned as an extreme group at all. Positioning yourself halfway between the policy of a hate group and a rights-centred group is not an acceptable position.
The Queensland service.
Some description of the Queensland service is provided.
It is described as an affirmative service, “which considers no gender identity outcome: transgender; cisgender or otherwise to be preferable”. The Vine review includes criticism of this approach, without recognising that the alternative to an affirmative service is a conversive approach, and without recognising that trans young people have a right to an affirmative service as a basic component of healthcare dignity and equality.
It makes space for the argument that “the initial assumption of gender affirmation may not be appropriate in the developmental context of children with differing presenting histories, where there may be uncertainty on the part of one or both parents or a lack of clarity regarding diagnoses”. These arguments are presented as acceptable reasons for wanting a non-affirmative service, without considering the significant harms that would result.
The level of assessment required is a potential concern (for me, not for the Vine Review, the Vine review wants more of this) (90 min intake assessment, to be followed by a bio-psycho-assessment (of unstated length) before being taken to MDT panel for decision making.
The description of the MDT panel is a potential concern (for me, not for the Vine Review, the Vine Review wants more of this). It notes that all staff in the service are part of the MDT panel and “”medical treatment will be offered where all members of the multi-disciplinary team agree that treatment is in the adolescent’s best interests as confirmed at a multi-disciplinary case review”.
This emphasis on requiring unanimity is a concern, especially noting the significant risk that this places on a service. Even just one gender critical clinician could prevent all gender affirmative care in this model. I’ve seen this happen in several locations.
And beyond this specific risk, why are large teams of clinicians by default required to take joint decisions on access to a simple form of healthcare. It seems like a defensive practice model of shared responsibility, rather than centring what is best for an individual service user. It also reinforces complexity and the need for not just one clinical judgement, but many clinical judgements, taking us further away from the idea of informed consent and decision-making removed from clinician gatekeeping and control. Why would multiple professionals, some who have never met the adolescent, be required, by default, to hold power over their access to healthcare [Note, this is not an argument for them to all meet and question the adolescent, this is the UK model and is even worse].
The average waiting time in 2024 was 505 days.
The model of care in Queensland is described thus:
The draft model of care describes QCGS assessment as including: (a) mental health risk assessment in the SSFT session, initial MDT care review and as required; (b) gender assessment after SSFT; (c) physical health screening if PB or GAHT is being explored; and (d) neurodevelopmental/cognitive assessment if diagnostic clarification of neurodevelopmental disorders serves a functional purpose for QCGS assessment.
Interventions focus on: (a) single-session and brief interventions; (b) risk assessment and crisis interventions; (c) pharmacotherapy; 191 QCGS Service Evaluation, pages 50 – 52. 192 Work Instruction as effective 5 February 2025 page 4. Work Instruction as effective 21 February 2024 page 3. Independent Review Advice Report 63 (d) interventions that promote parental/system capacity to coordinate care quickly; (e) education on gender diversity; (f) advocacy; (g) support with social transition; (h) chest binding; and (i) care coordination
Data on service numbers are on page 63.
Dealing with cisnormative parents
A review of this nature seems entirely ill-equipped to deal with input from transphobic, cisnormative or uninformed parents, even though this input is entirely to be expected.
Quotes like this are provided:
“some parents, described feelings of grief or loss when their child persisted in their TGD identity, and that those parents did not feel their experience was recognised”.
“some families, described feelings of concern that affirmation was seen as the inevitable and desired outcome, and that there was insufficient consideration of alternatives to PB and/or GAHT”
One role for services such as this is to educate and inform parents, whilst centring the need and rights of the child/adolescent. The Vine Review and similar reviews needs to centre the healthcare rights of children through this process. It should have expected some amount of feedback from parents who would rather their child had conversion therapy, and this feedback needs to be noted, but not be accepted as meaningful criticism of the current service model.
In a world where parents are at different levels of knowledge, holding different levels of prejudice, it is never possible for a service to meet the expectations of all parents. Critique needs to be reviewed through a lens of a commitment to depathologisation and trans and child rights.
“from some service users, that the typically slow assessment process was an endorsement that the assessment of the young person and their family was thorough, though others considered it overly cautious”. Again, the Vine Review is taking this as differences of opinion, whilst not recognising that some parents want their child to be grilled and challenged on their trans identity, while other parents want do not want their child to be put through unnecessary grilling.
I don’t like the way that the Vine Review groups parent and child together as ‘service users’, without clearly distinguishing when an opinion is from a child vs from a parent. Were the children actually saying that they were pleased with the thorough assessments?
On Data
“from some individuals, requests for long term follow up data collection to be made mandatory, and others concerns about privacy and opposition to being forced to participate in research or a trial”. Again, the Vine Review is hearing from different groups here. Trans young people have a right to data privacy and should not be forced into long-term research. Healthcare services need to uphold patient rights.
Two other important points noted in ‘panel heard in consultation’ boxes:
“concerns that a sole focus on gathering data to increase the evidence base may be at the expense of people that currently need treatment”
“that decreasing access to the treatments would result in large scale data being difficult or impossible to access or obtain”.
Reasons to not diagnose as per the Queensland service spec
(a) the young person not being TGD; (b) the young person having no dysphoria in relation to their body (no diagnosis of gender dysphoria); (c) the young person being ambivalent about starting hormone treatment; (d) parental disagreement; (e) the person being too young (pre-pubertal); (f) the person being unable to consent (for example, due to the impact of mental illness such as psychosis or if the young person is assessed to not have capacity); (g) the treatment being not safe socially due to factors such as unstable accommodation or out of home care; or (h) other medical risk.
Private providers
There is reference to private providers (P,68-69). Does seem to potentially be setting sights on restrictions there…
UK and Finland
The Vine Review panel looked to UK and Finland, two of the worst locations in the whole world, for input on alternative models. What a surprise that they stumbled upon that combination. Noone would assume UK + Finland is the ideal comparator for Australia – this is clear an indication of anti-trans influence.
On p,70 the JBI literature review describes “several European jurisdictions have moved toward more precautionary, research-based approaches”. This is false. The shift in places like the UK has nothing to do with caution or the wellbeing of young people, nothing to do with research-based approaches (the new approach has no research to back it). Their shift is everything to do with ideological and prejudice impacting on healthcare. The JBI summary is inaccurate.
Prejudice
Again, there is no recognition of the role of prejudice in this description “reports from the USA (DHHS Review and Utah Review) reaching different conclusions” (p.70). The DHHS Review did not just happen to come to different conclusions. It was ideologically established in order to remove access to trans healthcare. The Vine Review is trying to avoid any recognition of the role of prejudice in this field.
Expert opinion
It is really interesting that the JBI report takes expert opinion as sufficient to underpin guidance that raises barriers to care (on the need for comprehensive assessment and an MDT) but insufficient when it comes to access to care (on the importance of blockers or HRT).
Some of the sections quoted from JBI report 2 (that I haven’t read yet) are really problematic (p.70-71).
Professional liability
p. 76 has an interesting section on liability, that defines care as meeting acceptable standards where it “was widely accepted by peer professional opinion by a significant number of respected practitioners in the field as competent professional practice”. Professionals seem to be being pushed into ever more comprehensive (and abusive) assessment in a shift to defensive practice – professionals at Auspath were discussing documenting assessments in ever greater detail in case of legal cases where they needed to prove that they had indeed assessed everything. From the content in this section it does seem that another option would be possible – for Australian professionals (in significant numbers) to instead commit to rights-based practice, removing the need for this defensive practice emphasis on defending the comprehensiveness of an assessment and diagnosis.
This section doesn’t even consider the ethical dimensions of denying access to necessary healthcare.
Conversion therapy
There is a section on conversion therapy that entirely fails to consider when psychological therapy would cross into the territory of conversion therapy. It is quite bizarre how this isn’t even dealt with. Apparently, the legislation “does not prohibit any practice that is based on reasonable clinical decisions about how to provide safe and effective care”. A lot, it seems, hangs on the world ‘reasonable’.
It states “The Panel concludes that clinically appropriate full assessment of a person’s gender identity and any dysphoria related to that identity with no preferred identity in mind that aims to facilitate care and/or to support a person in managing the psychological impacts of their gender dysphoria/incongruence, should not fall within the definition of ‘conversion therapy’ above.”
Again, ‘clinically appropriate’ is something that needs to be understandable to make this legislation any form of actual protection for trans kids. I wonder if AUSPATH will write something on what is not clinically appropriate in terms of talk therapy or assessment for trans kids. This is even more important in services that are unable to offer any support for medical pathways, because those services will need to fill their time doing something.
Human rights
p.83 has a section on the human rights legislation impacting on healthcare. I will mention here my recent article with Ruth Pearce on trans childrens’ rights.
The right of trans children to access trans healthcare is waved away through reference to the lack of consensus and the lack of rigorous enough evidence that trans healthcare is an effective ‘treatment’ for the mental health disorder of gender dysphoria. The Vine Review did not start with anything like enough understanding of the historical and clinical pathologisation and psychiatric control of trans communities, and this can be seen in this section.
Privacy
The section on privacy comes from the perspective that it is a shame that trans kids have privacy rights. It seems to suggest that privacy and health data rights could be overcome if only PB and HRT were defined as ‘monitored medicines’ – medicines that are considered as potentially presenting a high risk of harm to patients…
Woe for criticised professionals
Here (p,89), as we saw in Cass, one section focuses on how hard it is for professionals if they get criticised or investigated for not being affirmative. There is no recognition of the harms of non-affirmative practice, the huge power imbalance between child and clinician and the lack of accountability mechanisms. This section also did not talk about the protection for clinicians who are attacked (often backed by Right wing funding) for being affirmative.
Risk of not
p.90 “The risks and benefits of not intervening must also be carefully weighed, including the ongoing impact that some participants described of developing irreversible and unwanted secondary sex characteristics which contribute to enduring distress into adulthood”
But that sensible statement is followed by this one:
“medicating otherwise physiologically healthy children and adolescents to help in managing their internal distress in the face of wider societal misunderstandings of gender diversity may create a disproportionate and indefensible burden on them”.
Ew Vine Review
Diagnosis p.90 deals with diagnosis very poorly. It contrasts patient autonomy with ‘diagnostic certainty’. But at no point does it deal with the fact that ‘need for puberty blockers’ or ‘need for HRT’ really can’t be diagnosed. The diagnosis of gender dysphoria is a very vague diagnosis anyway, and those hiding behind ‘diagnostic certainty’ are lying to themselves or others. Need for trans healthcare comes from listening to the individual patient and helping them take informed decisions – it is not a medical condition to be diagnosed with certainty.
Stigma
p.91 has a whole section on stigmatisation, marginalisation and discrimination, without once mentioning pathologisation, psychiatric control, or healthcare violence towards trans people.
Funding
“Allocation of funding is premised on a condition that interventions are effective”. “Services must demonstrate efficacy to justify continued funding” Here the terms are set up for defunding healthcare that is not deemed effective. Trans healthcare is one of the most effective and cost-effective areas of healthcare, with very high patient satisfaction. But here a lack of high quality evidence can potentially be utilised to defund such care.
P, 92 “Analysis, review and reflection on outcomes is therefore critical to justify ongoing funding which is appropriately targeted to achieve the best short and long term health outcomes for the diverse group of young people increasingly presenting to Queensland HHSs with gender-related distress.”
No centring of trans children and trans adolescents. Here we have young people with ‘gender related distress”. And who knows what ‘treatment’ best resolves ‘gender related distress’. Maybe denial of trans healthcare…. Maybe talk therapy… Maybe shaming kids back into the closet.
Diagnosis
Again (p,92), some of the boxes in this report are actually good.
“views that a diagnosis is pathologising and a source of oppression, and that medicalisation of TGD identities is unnecessary and stigmatising”
“that diagnosis is a barrier to access to treatment and should not be required to access GAHT treatments – some individuals reported that a desire for treatments of a child with agency is sufficient justification”
“that adolescents can experience less dysphoria than required by the diagnostic criteria but still want and may benefit from PB and/or GAHT, and may be unfairly excluded from treatment in the public system if diagnosis is used as an essential criterion”
Though some junk in there too..
Some of these boxes don’t seem to influence the core report conclusions at all. It is interesting which evidence and input shapes the report conclusions and which is noted and then side-stepped
Trans broken arm
The report acknowledges trans broken arm syndrome (p. 94) but then immediately talks about the opposite, diagnostic overshadowing.
P,95 has this absolute bullshit “Our view is that a person/child centred approach warrants the full assessment and early management of any co-occurring conditions before initiation of PB or GAHT.” This is not justified at all. There is no gold standard evidence of this requirement, that is pulled from the sky.
Noticeably this appears in a section referencing neurodiversity.
Coercion
I actually laughed out loud at this one. There is exactly one use of the word ‘coercion’ in this report. In a report on trans healthcare, an area of medicine that has historically been exceptionally coercive to young people.
This is the one acknowledgement of coercion (p,96): “The Panel also heard perceptions that a coercive environment is created when unquestioning gender affirmation, with or without access to PB or GAHT, was expressly linked to reduced suicidality for young people experiencing gender-related distress”.
Recognising the very real risk of hopelessness and suicidal ideation/attempt in young people denied essential healthcare, is the one place where the Vine Review talks about coercion.
Wow.
It then moves to look at Finland as a model. A place where the reports of healthcare violence and coercion from young people are off the charts.
Why do you think the Vine Review finds Finland the go-to model of healthcare for Australia? Is this common in other areas of Australian healthcare? Or is this a bit of an unusual reference point. The Finland state system is one of the last places I would look for advice on good healthcare for trans children.
Diagnosis
p.96 we are back to diagnosis.
Here more of the reasons to not want a diagnosis of gender dysphoria are covered.
The reason for wanting access to trans healthcare based on ‘felt need’ are mentioned. These are dismissed on practical grounds of needing to rationalise health expenditure (an argument entirely different to the argument around accurate diagnosis above). This statement is made “The practical necessity of the diagnosis of gender dysphoria as a pathway to treatment is acknowledged by some critics of the use of diagnosis.” One citation is provided. If you read that citation, it explicitly argues against gender dysphoria as a diagnosis, considering it outdated and pathologising. It suggests that the principle reason for utilising the more acceptable gender incongruence diagnosis is because a ‘term’ is needed for reimbursement purposes in diagnosis-oriented health insurance systems. This article does not upholding the need for a psychiatric diagnosis of which people suffer acute enough gender distress to access trans healthcare and it is misrepresentation to present it as evidence of ‘the necessity of a diagnosis of gender dysphoria.
This section would do well to consider parallels with other areas of health based on bodily autonomy, including abortion care, pregnancy care and reproductive healthcare. There is a reason why the revised ICD diagnosis has moved to reproductive health rather than psychiatry.
Social transition
“For some young people, social transition is an active step in managing gender dysphoria”.
This is so messed up. This is what happens when trans existence is framed through the lens of psychiatric treatment. Trans people aren’t socially transitioning to “manage gender dysphoria”. They are socially transitioned to stop hiding who we are and to embrace life authentically and with gender euphoria. Putting a psychiatric treatment lens on social transition is bad form Vine Review.
(this also opens the door to defining it as a medical intervention, needing clinical permission, as we are seeing in the UK)
“While social transition is physically reversible, the ongoing psychological benefits or harms are not yet fully understood”
No Vine Review, you don’t get to have opinions on the psychological benefits of using a new pronoun. Get in your lane.
P,98 Social media
This section is problematic. The word grooming is used to reference affirming communities on Reddit. It is unclear if they are referencing risk of actual grooming, using this term to talk about affirmation. Instead of centring the actual risks trans young people can face with social media, alongside the sizeable benefits, the focus is on parental experiences of being called transphobic for wanting to question or challenge a young person’s identity.
Affirmation
P,99 has a whole section on how affirmation shouldn’t entail using a young person’s pronoun or “an immediate acceptance of the gender the young person reported”. Gross. The Vine review here moves into wanting non-affirmative practice dressed up in the language of affirmation.
If you accept “consider no gender identity outcome to be preferable”, then of course you will accept and not problematise the gender that a young person describes themselves as.
If you problematise and do not accept the self-description of a young person, but only when they are trans (assuming you don’t do this in clinical practice with cis kids), then you are clearly suggesting there is a problem with a trans identity.
Why is the Vine Review trying to change the accepted meaning of affirmative care, and trying to push for non-affirmative approaches through the back door?
“outward facing symbols may lead to premature foreclosure or ‘settling’, potentially limiting ongoing genuine exploration in the child’s best interests”. Love it when the psychobabble comes in. Premature foreclosure indeed. Genuine exploration in the child’s best interest. Hmm.
P.100 I’m going to stop here, cos this is already ridiculously long. Why are all these healthcare reviews both a) so long and b) so bad that it takes pages of notes to even scratch the surface with what’s wrong with them. One final point
Systematic Reviews and Qualitative Literature
I looked briefly at the JBI literature review that underpins the Vine Review. It is yet another Review of Evidence that claims to be comprehensive, that claims to include qualitative literature, that yet again is absolutely terrible at it, excluding nearly all the qualitative literature. It is really not good enough to claim to cover qual literature, and to conclude that there is only one (not peer reviewed) qualitative study on puberty blockers. The fault here comes down to a lazy search strategy.
Here they search three databases, all focused on psychological or bio-medical literature. The first two databases exclude the majority of qualitative literature. PubMed only include literature funded by major funders, which is likely to include the bulk of expensive clinical studies, but largely excludes inclusion of qualitative literature which is less likely to receive big institutional funding. Embase focuses on biomedical journals, and does not include the many qualitative healthcare experience articles that are usually published outside of biomedical journals. The third database, Psych info, focuses on psychology and social sciences. It does appear to include a greater range of qual relevant journals. It is strange that the authors of the JBI literature review claim to have done a comprehensive search of Psych info, and yet to have found zero peer reviewed qualitative articles on the topic of puberty blockers. Is this a problem with the database Psych info, or did the authors fail to do a proper search for qualitative literature? I cannot access the Psych info database search, so I can’t test whether more of the qualitative literature, including my own work, appears in there.
It is a recurring pattern in trans healthcare that literature reviews that claim to be comprehensive, that claim to include qualitative literature, fail to find that literature, often finding one or two articles at most, when there is a huge body of qualitative literature on trans health.
In late November I attended the AUSPATH (Australian Association of Transgender Health) conference in Tasmania, Australia. I had been invited as the key-note speaker on the first full day of the conference, given a 50 minute slot (followed by 40 min panel discussion with head of WPATH and head of PATHA (New Zealand Association of Trans Health). The audience was 555 people invested in trans healthcare, mostly trans healthcare professionals and advocates from across Australia, with a 50+ contingent from New Zealand. For transparency, as an invited key-note speaker I had my travel and accommodation paid by Auspath – I did not receive any other payments. A few people have asked if I can share my presentation – it was not recorded but I have captured a lot of the presentation content here, a mixture of my notes and memories combined with some of my slides.
Hi everyone, I’m absolutely delighted and honoured to be here today. I’ve already learned a lot about Australia in just a few days – I’ve learnt what a drop bear is. I’ve understood that my taste in Australian beer (VBs) is apparently bogan.
My name is Dr Cal Horton, I’m a trans and non-binary researcher from the UK. I’m also a parent of a trans kid. Being an advocate for and parent of a trans kid is not a particularly great position at the moment in the UK, so I will ask for no photos today please. I am currently based at both Oxford Brookes University and University College London. I am actively looking for routes out of the UK for my family, so if anyone is looking to hire a researcher, get in touch. I have no declared conflicts of interest – big pharma hasn’t come knocking yet – any day now, I’m sure.
Before I begin my presentation, I want to start with a reflection on the time and place at which I’m talking. In terms of place, I want to acknowledge the Muwinina and Palawa people as the traditional owners of this Land. I recognise histories of violent colonialism and brutal dispossession, and pay my respect to Aboriginal Elders past and present across Lutruwita. Sovereignty was never ceded, this was and is Aboriginal land. In terms of time, I recognise that we are speaking following two years of live streamed genocide in Palestine. In the UK we have a long and brutal history of colonialism and violence against marginalised groups. I note that this year the Lemkin Institute for Genocide Prevention raised a red flag warning for risk of genocide for trans and intersex communities in the UK.
Today my presentation is going to focus on how we move from pathologisation and violence to autonomy and rights in trans healthcare, with a focus on trans children. I’m using the term trans child to refer to everyone under the age of 18, though will sometimes reference more specific terms like trans adolescents where relevant.
When I talk about why the UK is so bad for trans people, why it is so bad for trans children, and for trans children’s healthcare, it is important to talk about the three Ps. Firstly Prejudice. We have a situation where individuals holding acute prejudice about trans people are in positions of influence or leadership over trans children’s healthcare. We have individuals in charge of the new children’s gender service who have never even attended WPATH, yet who have found the time to attend events organised by misinformation groups recognised as anti-trans hate groups.
The second important P is Pathologisation. In the UK you never even here the term ‘trans child’ in our NHS. It is all ‘gender questioning children’ or ‘children distressed by their gender’, ignoring the reality that the major reason that trans children are stressed and distressed is because of the violent persecution they are facing, including from the NHS. The language in the UK always focuses on describing trans children in pathologising terms, describing them as a group that are “complex” with extensive “co-morbidities”.
The third P, that impacts on trans children’s oppression in the UK, is Power. The current situation for trans children in the UK, the current situation for trans people in the UK, is impacted by the systemic exclusion of trans people from positions of establishment power, across and beyond the NHS. In my work, understanding why everything is stacked against trans children, I’ve started to increasingly focus on the concept of cis-supremacy.
When I talk about why the UK is so bad for trans people, why it is so bad for trans children, and for trans children’s healthcare, it is important to talk about the three Ps. Firstly Prejudice. We have a situation where individuals holding acute prejudice about trans people are in positions of influence or leadership over trans children’s healthcare. We have individuals in charge of the new children’s gender service who have never even attended WPATH, yet who have found the time to attend events organised by misinformation groups recognised as anti-trans hate groups.
The second important P is Pathologisation. In the UK you never even here the term ‘trans child’ in our NHS. It is all ‘gender questioning children’ or ‘children distressed by their gender’, ignoring the reality that the major reason that trans children are stressed and distressed is because of the violent persecution they are facing, including from the NHS. The language in the UK always focuses on describing trans children in pathologising terms, describing them as a group that are “complex” with extensive “co-morbidities”.
The third P, that impacts on trans children’s oppression in the UK, is Power. The current situation for trans children in the UK, the current situation for trans people in the UK, is impacted by the systemic exclusion of trans people from positions of establishment power, across and beyond the NHS. In my work, understanding why everything is stacked against trans children, I’ve started to increasingly focus on the concept of cis-supremacy.
Thank you for listening.
My wider reflections on AUSPATH are available here:
Last week I had the huge privilege of being invited to give a keynote speech at this year’s Auspath (Australian association of transgender health) conference, held in Tasmania. I loved being at Auspath, met many awesome people, and enjoyed learning about Australian approaches and best practices, many of which I wish the UK would learn from. There were also a couple of things at Auspath that gave me pause. In this blog I’m going to briefly run through some of the things I liked best at Auspath, before a deeper dive into two areas of that left me thinking. I don’t claim to have all the answers, but am sharing my current thinking – I would love to hear other people’s takes, on their experience at Auspath, on their priorities for improving trans youth healthcare in Australia and beyond, and on their experience and perspectives on the two issues covered at the end of this blog.
Highlights
It was a rare joy to be around so many incredible people fighting hard for a positive future for trans kids. I really valued:
Hearing so many clinicians speaking with genuine compassion and respect about trans lives. Even where I took issue with a minority of clinical approaches, the professionals I heard at Auspath clearly cared for trans youth, clearly had a base level of respect for trans lives, clearly wanted the best. It is a very different world from the UK where I can count on one hand the number of NHS professionals I’ve met who I’ve heard speak respectfully about trans kids. I’ve focused the latter sections of this blog on critique rather than praise, because pretty good shouldn’t be the bar – Australia has the potential to be world leading in trans youth healthcare.
Hearing so many professionals, advocates, community members, parents, allies, speaking with determination about protecting trans kids and trans healthcare from the abuses spreading across the world.
Hearing an impressive and eloquent young person speak about their experiences, including obstacles and barriers to equal access to healthcare.
Hearing an impressive and eloquent parent share their experience on the difficult path advocating for a trans child in Australia.
Learning about Country and first people’s knowledge and experience. It would have been good to hear more on the topic of first people’s experiences and priorities.
Listening to a panel talk about the fight for trans kids in Queensland (I was crying through most of that panel).
Feeling really welcomed at the conference, some many people came up to me with kind and friendly words, and I also felt very welcomed as a non-binary person in that space.
Hearing a panel of young adults speak on their experience advising on trans health research projects, on the need to include young people who were unable to access paediatric services, the need to include rural youth, the need for fair pay, for both career development opportunities for those who are research inclined as well as keeping space for input from young people with no interest in working in research. The importance of disability justice informed approaches.
Meeting young adults who are willing to challenge establishment status quo approaches. I think this is really valuable. So much cis-supremacy and cisnormativity operates through the maintenance of outdated systems and approach that we don’t even question. Having young people speak up and ask these questions is super important. One such question was ‘do we ever need to collect and report on data on assigned sex/gender?’. It’s a really good question. My current answer is ‘I don’t know, but certainly very significantly less than we do at present. This is definitely a question I will carry with me. I’m doing a new piece of research at the moment on non-binary adults and in that survey we are including a specific question ‘do you want to see results from this research broken down by assigned sex/gender?’, along with open text boxes for people to share their reason for or against. These answers should likely be context specific and driven by the information needs of the people whose data it is. Certainly we should have already moved away from the approach I still saw some places in Auspath where a person was introduced as ‘patient A – AFAB – identifies as a boy’.
Meeting lots of awesome people from New Zealand, commiserating and strategizing on how to fight and support young people through state enforced discrimination.
Meeting lots of healthcare providers working outside of specialist gender clinics, who are working to develop alternative routes to respectful and informed consent care. Many of these are currently supporting adults – with confidence and advice the same care can be extended to under 18s.
There were two points in Auspath where I heard completely different messages from different people, and that relates to the two topics that I’d like to do a deeper dive into in this blog: MDT assessment and comprehensive bio-psychosocial assessment. Some people came up to me and expressed concern that such things were happening in the UK, and that we should fight them being introduced in Australia. Other people came up to me to share their knowledge of these practices being experienced by trans children in Australia.
In my presentation I spoke about the harms of excessive questioning of trans kids. In the UK this 100% comes from a position of bad faith. Clinicians are encouraged to ask hundreds of questions, with an intention of probing, prodding and undermining trans identities. At Auspath I did not hear any explicitly and intentionally bad faith or actively transphobic intent. I did however, from some clinicians, hear approaches that, whilst coming from a better place, constitute the same excessive questioning. In Australia this excessive questioning was sometimes marketed and justified as ‘adding value’. Even from some brief conversations with service users I heard people share stories of having experienced this ‘added value’ as harmful. I would really like to call attention to the over questioning of trans kids even in nominally affirmative services. Being trans is normal, and trans kids shouldn’t be faced with extensive additional healthcare questioning compared to their cis peers. Any systems that normalise asking additional bio-psycho-social questions of trans kids compared to what is standard for cis kids is a problem. And here, our base comparator should not be the among of questioning that is standard for cis kids who need psychiatrist or psychologist support – our comparator should be an average cis kid who is not under psychologist or psychiatrist led care. Simply being trans, or accessing trans healthcare, does not justify invasive and excessive psychology centred questioning – this approach is a legacy of pathologisation. Two phrases were heard at Auspath more than I would like: Multi-Disciplinary Team Assessment, and Comprehensive Bio-Psycho-Social Assessment.
Multi-Disciplinary Team Assessment
In the UK it is presumed that a trans child needs to be assessed by multiple different professionals, often including a psychologist, psychiatrist, paediatrician, social worker, and that is before assessments with an endocrinologist or fertility specialist. These multiple levels of assessment are abusive and excessive. At Auspath clinicians listed a dizzying array of different professionals being involved in MDT assessment of trans kids. In Spain, in the highly respected Transit service in Catalonia, trans kids see one medical professional, usually a GP. The GPs role is to support informed decision making by a trans young person (and their family depending on age), their role is not to assess and decide upon access to healthcare. In this Spanish service that one medical professional, that one GP, can provide healthcare, including endocrine care for trans adolescents, without input from additional professionals. They do still operate in what they describe as a multidisciplinary team, having different colleagues within their service. This multidisciplinary team allows the GP to offer access to different additional services, optionally, in an opt-in approach. Young people can ask to additionally see a psychologist. They can ask to see a social worker or family worker, to support with school for example. But these additional professionals are additional optional services, a trans young person does not have to see, and certainly does not have to be assessed by, a whole multidisciplinary team of different professionals.
At times in Australia it was unclear to me what different clinicians mean when they refer to multi-disciplinary team working. I hope Australian colleagues can consider and articulate where they are working within an MDT that offers optional opt-in access to a range of different professionals, without mandating that a trans child see an overwhelming range of different professionals. I hope clinicians can be clearer in whether their approach forces trans young people into running a gauntlet of different stages of assessment by a series of different professionals. I hope more attention can be drawn to the harms of forcing trans children through multi-professional assessments where additional professionals are not desired or needed. WPATH SOC 8 recommends an MDT assessment for trans adolescents – I hope Australia can be part of building an evidence base for a better approach in time for SOC9.
Comprehensive Bio-Psycho-Social Assessment.
This is a term that I find really triggering. In the UK this term is used to define practices that are pathologising, intrusive, uncomfortable, and harmful for a trans child. When I first heard this term from clinicians in Australia I assumed it meant something else here. I initially hoped that it was being used as a defensive practice, by clinicians under anti-trans pressure, who are keen to emphasise the thoroughness of their care, using this term as a fancy descriptor for actions that I, as a non-clinician, would describe as ‘having a chat’, or ‘getting to know your patient’. A good GP can ‘have a chat’ with a patient, and quickly find out some useful information about them to better help them understand, build rapport with, and support their patient. This can include some brief questions to understand their life circumstance, their family support, their strengths, supports, stresses or concerns. This can be done rapidly in a first appointment as a non-intrusive, flexible, patient-centred and low stakes chat. This should not be defined as a ‘comprehensive bio-psycho-social assessment’.
I was chatting to one clinician, who described taking notes during such a ‘getting to know you’ chat, with those notes not affecting care pathways but being taken primarily to enable quicker rapport building at the next appointment. I commented that I find it really uncomfortable to have clinicians take notes when I am asked questions about my life and circumstance. This is clearly linked to my own institutional trauma in unsafe healthcare settings where answers to these questions are definitely being judged by clinicians, where answers might end up in a non-consensual case study report, and where these notes do impact on your (or your child’s) access to care. It is important for good healthcare professionals to note how much institutional trauma and distrust many trans people, including trans kids, carry into the clinic. Even young people I met in Australia spoke at length of trauma experienced in encounters with various healthcare professionals who were there to judge and control.
I had initially hoped that references to ‘comprehensive bio-psycho-social assessment’ were just a sign of defensive practice. I was dismayed and at one point upset to hear that actual comprehensive bio-psycho-social assessments are still a core part of care in locations across Australia, particularly in trans children’s healthcare, particularly in services delivered by mental health professionals. I was disappointed to see reference to incredibly detailed family tree mapping, filled with details entirely unrelated to a child’s access to trans healthcare services. I was disappointed to see wide-ranging body mapping exercises, children asked to draw themselves, notes taken on left or right handedness, even assessments of pen grip. Many of these unnecessary and pathologising over-assessments were marketed and justified by professionals as ‘adding value’. If we are seeing a trans kids, we ‘might as well’ assess whether they are having trouble holding a pen. We might as well investigate their full family system for areas of family disfunction. We might as well screen for ADHD, autism, anxiety, anger issues, dyslexia, poor family functioning, disordered eating, sexual health support needs, bullying support needs etc etc.
The list of things we ‘might as well offer’ as ‘added value’ while we are here grows ever longer, especially in trans children’s healthcare. Some of this emphasis on ‘added value’ is perhaps a symptom of some professionals realising that the original reason for their role is outdated, pathologising and unneeded. But why are ‘added value’ assessments brought into trans children’s healthcare? Why are trans children’s healthcare assessments so broad, ill-defined, all encompassing? The answer lies in services that are struggling to adapt from a pathologising model of care.
In terms of unnecessary questioning added on to trans healthcare, I am perhaps least worried about short screening questions that are designed to triage young people to additional support services that might well be beneficial. Some trans kids might also want an ADHD assessment. Some might want support for anxiety. But even then I’d rather this was done transparently, optionally, and with patient consent ‘would you like to do a few additional questions to help us see whether you might benefit from our optional mental health or neurodivergence services including related to anxiety, ADHD, eating disorders etc. For triaging child developmental concern, this can be similar ‘while you are here, would you like us to check your/your child’s pen grip, for dyslexia etc’. This transparency is important as it helps service users understand and have trust in the process, while also letting them tell clinicians when ‘added value’ services are not need, are already being managed by other professionals or are not wanted at this specific time. Crowding all types of assessment into a trans health assessment makes these extra long and stressful.
Then there are areas of a comprehensive bio-psycho social assessment that are clear remnants of past pathologising models. Questions on childhood toys, friendships, family gender roles, sexuality of parent or child, and many other unnecessary questions are inappropriate. At the conference there was one exchange that was particularly noteworthy. A clinician commented that they always ask trans young people about their romantic relationships. They noted that young people commonly respond by querying ‘why are you asking this?’. They said that they then tend to respond ‘Because it helps remind me that you are a full human, more than just your gender/transness’ (I didn’t take live notes and won’t be getting the statement 100% accurate).
I had three reflections on this answer. Firstly, it is important to recognise power dynamics in a clinical encounter. It is hard for any service user to question the approach of their clinician. It is particularly hard in a trans healthcare appointment, and especially so for a child. If young people are questioning our approaches, we would do well to take this as a significant potential indicator of discomfort. It is really hard for a child to question an authority figure, especially one whose approval they need. If we are asking questions that young people indicate some level of discomfort with, if there is not a very strong clinical need, surely we should not be asking those questions.
Secondly, I note that the young person’s question ‘why are you asking this’ was not provided a satisfactory answer. Clincians should not need private information on trans people’s lives in order to remember that we are more than being trans. I don’t think the speaker realised the impact of their words on some trans people in that room. I left the room at that point. There is a long history of trans people, especially trans kids, being asked invasive questions for no reason other than to satisfy clinician curiosity. Curiosity driven questions are entirely inappropriate – we shouldn’t have to humanise ourselves in order to access healthcare.
Thirdly, sexual orientation and relationships questions are often asked without clear purpose. In the UK these questions are deemed necessary based on anti-trans fake theories of childhood transness being a reaction to homophobia or sexual abuse. In the UK’s puberty blocker trial these are also justified through inclusion of a criteria excluding youth with any judged potential for having unprotected sex from eligibility to access the trial.
In less transphobic services these questions are sometimes justified by reference to a need to screen for unmet sexual and reproductive health information and support needs. I would tend to agree that trans youth may have unmet sexual and reproductive health information and support needs. Schools, regular resources and parents may all be ill-equipped to provide trans-inclusive education. But screening for unmet sexual and reproductive health needs can be done transparently, intentionally, none creepily and with consent. It does not need to be untransparently sneaked into a wider trans healthcare assessment, where historically youth have been forced to answer unwanted and intrusive sexual questions driven by clinician curiosity or clinician ignorance, unrelated to screening for sexual and reproductive health services. I would suggest that asking a young trans adolescents about their sexual and romantic relationships or desires is rarely an effective strategy in building rapport. When asking potentially irrelevant questions that are likely to make a young person uncomfortable it is not sufficient to give them an option not to answer. Some questions should not be asked. I’ve accessed specific sexual and reproductive health services as an adult without being asked any of the type of personal questions that psychologists and psychiatrists sometimes feel entitled to ask of trans children.
I would strongly question the appropriateness of insisting on a comprehensive biopsychosocial assessment in trans youth healthcare. I would ask clinicians to document much more clearly the questions they are asking and the purpose or clinical need for each question. I would suggest tat rapport building questions should be short, comfortable, flexible and non-intrusive. I would suggest that ‘added-value’ screening questions to triage to additional support services should be transparent, opt-in areas of questioning, strongly delineated from what is being assessed.
I hope we can quickly evolve away from assessment-based models of care for trans children and young people. And while assessment remains, we all have a shared duty of care to reduce the exceptionally excessive breadth and depth of questions that have become wrapped up in a comprehensive biopsychosocial assessment. Professionals who are able to deliver effective rights-respecting healthcare to trans children and young people in Australia without invasive psychological and psychiatric assessment as standard, please can you more clearly communicate what questions are actually clinically necessary, whilst also documenting the questions that you consider not clinically valid. (I’m happy to anonymously share examples on my blog).
Trans healthcare is not a psychological or psychiatric treatment, and we need to move trans children significantly further from being in positions of psychology/psychiatry-centred questioning and assessment. I’m not against jobs for psychologists and psychiatrists – we can channel those existing resources into helping trans kids with anxiety and stress related to living in a trans-hostile world, and into treating the adults around them who fall into anti-trans radicalisation. Trans kids in rights-respecting healthcare services across different parts of the world receive trans healthcare without a comprehensive biopsychosocial assessment, and we can aspire to this across Australia.
Flight home
After Auspath I tagged on a few holiday days in Tasmania, seeing some beautiful landscapes and wildlife, an incredible experience. I’m writing this blog whilst rather sleep deprived and time-zone confused on a long flight back to the UK. In the two weeks I was away, the UK has completely removed protection for non-binary people (in a legal case that made absolutely no sense); the UK has banned trans girls (and trans women as leaders) from girl guides; and banned trans women from the Women’s Institute. These are all severe blows. Girl Guides has long been one of the best allies for trans girls – an organisation whose inclusive policy we have long pointed to when asking for schools or other organisations to choose equality and inclusion. Having them bow to transphobic pressure is a blow not only for the impact on Girl Guides, but for what this means for the whole state of inclusion of trans girls in UK society.
I have felt so much lighter and safer being in Australia and fly ‘home’ with significant trepidation and fear for the future. At least I am re-energised from feeling safe and hopeful through my days in Australia and at Auspath. But the fight goes on.
Thanks to anyone who got to the end of a very long blog!
When puberty blockers were banned in June 2024, the legislation included a clause stating that those currently on blockers would not be medically detransitioned, and could continue care if adopted by an NHS GP.
Only one NHS GP practice, WellBN in Brighton, agreed to take over this care, with trans adolescents and families from across Great Britain moving to their care. Patients have reported extremely high rates of satisfaction with this care.
In May 2025 ICB Sussex (ICB = Integrated Care Board, the level of bureaucracy above a GP practice and below NHS England) and NHS England launched an investigation into this care. The investigation has already caused a high level of harm to trans adolescents and families. Essential care is under threat of being taken away, with a threat of forced medical detransition. One person (I can’t share their identity) put this situation into a series of illustrations, capturing powerfully the current situation. This has been shared on instagram, but for those who don’t use it, they gave me permission to share here. I’ve added a bit of extra context.
Image one captures the ICB’s allegation of trans adolescents having been exposed to ‘potential harm’. What we instead have seen, is young people thriving and excelling through access to respectful affirmative healthcare.
[Description of image 1 “Potential Harm”: One trans young person is winning at sports; One is dreaming of a happy future relationship and marriage; one is hanging out with friends; one is doing their school work; one is playing the piano while proud parents watch; one is going shopping with a parent – while professionals write up reports of potential harm]
Image two captures the NHS’s approach to data collection. GP practice patients refused consent for the ICB taking their private patient data. GP practice patients, adolescents and parents, added notes to their files formally refusing permission to share their data. The GP practice did not want to share this data, and refused for several months. The GP offered anonymised data – the ICB was not interested in anonymised data. The ICB and NHS England stated that consent was not necessary due to ‘patient safety concerns’ despite no evidence of harm. The ICB finally threatened to cancel WellBN’s whole NHS contract, closing down a GP surgery with 25,000 patients, if they didn’t hand over patient data. WellBN at this point folded and handed over all trans children’s data. Information commissioner office complaints have been submitted.
[Description of image 2 “Data Pulling”: A house is being trashed with objects broken. Men in black suits (with the words Multi-disciplinary team on their top) are forcibly removing boxes of data, while adolescents and families try to keep hold of them. The boxes are labelled ‘private data’, ‘gender history’, ‘medical history’, ‘childhood history’.]
The third image covers the evaluation of patient harm. A patient harm investigation is being conducted without speaking to a single trans adolescent or family. It is being conducted purely based on clinical notes. The conclusion has been pre-determined with the investigation clearly considering affirmative care inherently a form of harm. Trans adolescents and families have prepared testimony on the reality that not only has there been no harm, their care has been excellent. Trans adolescent and family voices are not being heard.
[Description of image 3 “Desktop Review”: Adolescents and families are shut outside, using loud speakers to say ‘Please hear us, we were not harmed’; ‘children not harmed’, ‘no harm only care’. Inside, behind thick walls sits the head of the investigation team doing a ‘desktop review’ writing ‘harm is evident’.]
The fourth image focuses on the ICB’s plan to close all WellBN Care and refer patients elsewhere. Trans youth who are under 17 are to be forced to into gender clinics that offer conversive talk therapies focusing on investigating trans identities. 17 year olds will join waiting lists for adult care that stretch into years and years long.
[Description of image 4 “Expedited Referral”: A scared young person is being pushed into a room. The room was labelled ‘conversion therapy’. The word conversion has been crossed out, and in its place the words ‘gender exploratory’ therapy are now scrawled. In another scene a slightly older adolescent sits at a computer where the screen states ‘Gender Identity Clinic waiting times: 75 years].
Image 5 covers the preferred NHS approach for trans youth, gender clinics that focus on invasive, traumatic and inappropriate questioning of trans youth.
[Description of image 5 “Holistic Assessment”: Worried looking parents embrace a worried looking adolescent on one side. Ahead of them is a barrier labelled ‘caution no treatment ahead’. Behind the barriers are six faces with word bubbles ‘how do you feel about your penis?’; ‘do you get erections?’; ‘how often do you masturbate?’; ‘Are you sure you’re trans’?’; ‘Do you like girls’ underwear?’; ‘are you gay?’].
Image 6 focuses on the ICB’s intention for ‘assisted withdrawal’ of affirmative healthcare. This is forced medical detransition. It is abusive and harmful.
[Description of image 6 “Assisted Withdrawal”: A trans girl is having her long hair cut and facial hair painted onto her face; a trans boy is having breasts added; a young girl musician is crying while a professional says ‘don’t worry you’ll be singing with the boys in no time’]
The ICB have stated that they expect the outcomes to be ‘stark’ for impacted trans youth ‘especially the younger ones’. This image powerfully captures the type of stark outcomes that the ICB is well aware of as possibilities, having included these risks in their own risk assessment.
[Description of image 7 “Stark Consequences”: The image shows various depictions of children and adolescents having serious mental health consequences, including school drop out, stopping eating, mental health crisis and death]
The eighth image captures the ICB and NHS England’s intended ‘robust tracking approach’. Now that they have full patient data on adolescent and supportive families, they intend to ‘robustly’ track these children and families, keeping their data for 20 years, and tracking what adolescents and families do next. They have stated that if they think families and adolescent will continue to access medication through private means, they will be reported by the ICB to social services. Families and adolescents feel extremely threatened, extremely unsafe. Many are trying to find ways to flee the country.
[Description of image 8 “Robust Tracking Approach”: A scary large figure with a magnifying glass stares down at a scared looking child, while parents try to pull the child away to somewhere safer]
The final image shows scared young people being pushed into a black hole.
[Description of image 9 “Improving Lives Together”: Scared young people, some of whom are crying are being pushed into a black hole. The adults pushing them in are saying statements like “just one of those stark outcomes”; “have to follow the guidelines”; “It’s not commissioned”; “the guidelines have shifted”; “there are trans kids?”; “the terms of reference sets this out quite clearly”.
Across all of the above images the artist has included ICB Sussex’s tagline ‘Improving Lives Together’.
The UK Government and UK research councils have contributed £10 million pounds to a series of research studies on service users of the newly established Children and Young People’s Gender Services.
These studies include the PATHWAYS study programme (Puberty suppression And Transitional Healthcare with Adaptive Youth Services) led by Kings College London in partnership with the NHS. This programme covers five different studies.
1) ‘PATHWAYS HORIZON’ is a longitudinal observational cohort study of all children and young people (n~3600) attending CYPGS.
2) ‘HORIZON Intensive’, encompasses a sample of those from PATHWAYS HORIZON who are not approved to receive endocrine care who will be more intensively studied as a control group for PATHWAYS TRIAL;
3) PATHWAYS TRIAL, a study of those approved to receive puberty blockers (GnRHa) as part of a research study.
4) ‘PATHWAYS CONNECT’ a study of cognition and brain development in CYP attending the services, including those who are and are not receiving GnRHa.
5) ‘PATHWAYS VOICES’ a longitudinal qualitative interview based study of CYP attending CYPGS. In this article we will focus only on the first study, PATHWAYS HORIZON.
Here I’m just focusing on the questions that will be asked under the first study, Pathways Horizon.
In this blog I want to do two things:
Highlight some big picture concerns with the questions asked in the PATHWAYS Horizon study, alongside some recommendations for families and young trans people engaged with the new NHS England and Wales Gender Clinics.
Outline in an accessible format all the questions that are being asked in that study, so that families and trans young people can be better informed on whether they choose to participate.
The PATHWAYS Horizon study hopes to gain the consent of 80% of young people and families to participate in it. I hope that number will be very much smaller. I do not believe it will add useful information to our academic understanding of trans young people, certainly not information that is worth the risks and harms inherent in the whole approach and service. I consider not participating in this study (or at least opting out of the more harmful tools) an act of harm reduction for trans children, young people and supportive families. When I was first given some of these exact same tools, many years ago, when I first attended a GIDS appointment as a naïve and unknowledgeable parent of a young trans child, I did not feel able to decline to participate in filling in questionnaires that made me feel really uncomfortable. I hope to empower others to make a different choice.
Big Picture Concerns
They are asking an excessive number of questions, which is itself abusive and unreasonable – over 314 questions are here listed.
A large number of these questions of more or less irrelevant or only tangentially relevant for trans kids – they are not clinically useful, necessary or meaningful
These questions will never demonstrate what healthcare benefits trans children.
The data collection shown here will be exhausting, time-consuming and expensive, a colossal waste of NHS and research resources whilst not delivering useful outcomes.
Many of the questions outlined below are deeply pathologising, invasive, trauma-inducing and inappropriate.
Several tools present trans children as a problem, potentially reaffirming parental biases, and potentially reinforcing trans children’s shame and self-hate.
I continue to recommend families to avoid the new service, as it holds very little potential of offering anything of value, and high potential to cause significant harm. For many families it may just end up being a significant waste of time.
If families choose to attend, hoping for the chance to be part of a puberty blocker trial, please think carefully before choosing to participate in this research. As an academic researcher specialising in this field, this planned research is not needed, will not lead to better care for trans youth, and in the wrong hands research of this nature can be distorted to further reinforce pathologisation, control and barriers to care. Participation in this research is not necessary to be eligible for the puberty blocker trial. Please know that you can decline participation. Please let your young person know they can decline participation.
If you do still choose to participate, please be aware of the potential for harm and trauma in several of the tools outlined below.
In particular I am concerned about the tools labelled the Child Behaviour Checklist (which is an awful tool to use for trans children, asking 118 questions on how much of a problem they are to the world), the Utrecht Gender Dysphoria Scale – Gender Spectrum (UGDS-GS) (which uses very outdated measures of gender dysphoria); Body Image Scale – Gender Spectrum (BIS-GS) (a horrific tool that asks children to assess how much they hate all their body parts); the ALSPAC Romantic Relations (which in spite of its name asks totally irrelevant and intrusive questions about the sex life of those aged 12-17). The SCOFF tool has a questionable name for a tool designed to screen for eating disorders.
I continue to be concerned about the questions that will be asked under the heading ‘medical history’, which by description is far wider a category with room to ask all kinds of irrelevant questions. I expect that component could include the typical gender clinic fascinations: many questions for parents on childbirth, parenting approaches, family deaths, family tensions, family gender roles and other irrelevant and trauma-uninformed lines of questioning. I expect there will be many questions for young people on defending and justifying their theoretical understanding of gender, and questioning them on proposed causes of gender confusion including social media, peer pressure, porn viewing, childhood trauma, parental homophobia or whatever is the latest transphobic focus in a search for anything other than transness to explain transness.
Throughout the years of the earlier GIDS clinic, there was a long and noble history of trans children, adolescents and supportive families putting the questionnaires that were offensive and harmful straight in the bin. Of asserting a right to not answer any question that feels off, that feels uncomfortable, that doesn’t seem relevant to the healthcare support being sought. Please continue this noble tradition in the new service. You should not answer any questions that make you or your young person uncomfortable. Bad questions always give bad data that will not benefit any trans young people. Research trauma is a serious concern. The NHS and associated researchers are not taking their ethical duty of care seriously, so we need service users to take this on. I’m writing this primarily to parents as I don’t think under 18s are likely to read this. But for any trans under 18s who do read this – please don’t feel pressured to answer questions that make you uncomfortable or seem strange or irrelevant. You do not have to answer and they cannot make you.
This is the non-intensive study – an additional ‘intensive study is also planned for those who will be in the puberty blocker trial and the control group for that trial). I repeat more than 314 questions for parents and more than 314 questions for children/young people is the non-intensive study.
These extensive, time and resource consuming, and largely irrelevant questions need to be understood in the context of a service that is trying to give the appearance of being busy, giving the appearance of doing something RIGOROUS, whilst failing to deliver any of the services that trans young people need and have a right to. It serves to keep service users distracted from the care that is not being offered. It provides baseline data on a host of largely irrelevant (or tangentially relevant) areas of mental health, generic well-being, neurodivergence etc, from which the service can seek to ‘further explore’ every one of those ‘issues’ or concerns, whilst denying or delaying affirmative healthcare. The type of intentional distraction and delay is a known component of modern conversive approaches.
Conversion therapy in the NHS never wears a badge saying ‘I will make you cis’. It comes much more subtly: Before we talk about the support that you need, FIRST we need to ask these hundreds of questions. Before we talk about puberty blockers or HRT, we first need to explore each of these areas of mental health or neurodivergence, or sexual attraction or family functioning or body image or sex life. We need to thoroughly explore what is going on holistically before we can do anything else. We need to be thorough. We need to avoid misdiagnosis. We need to rule out other causes. We need to Explore.
Not useful research: In spite of hundreds of questions, pages of spreadsheets and millions of pounds, this research will not answer questions that would be useful for a health service to know the answer to. Questions like: What are the things that make life harder for a trans child or adolescent? What are the things that improve things for trans children? The research isn’t answering these questions because we already know most of the answers. And our NHS and government and country does not like the answers to those questions. Cos they don’t care whether trans kids have a tough life. They don’t want to help trans kids at all. That is not the purpose of this service. It is a service to ‘study’ trans kids, to delay trans kids, and through delay to convert trans kids – pushing them to suppress their identity, to give up their fight, to think of themselves as a problem, as broken, pushing them to give up even thinking that they matter or have rights.
Number of Questions
Tool
Parent questions
Child/Young Person Questions
Kidscreen-52 (generic wellbeing)
52
52
CBCL (Problem behaviour)
118
118
Parental ‘About Yourself’ Questionnaire
2
0
SNAP-IV tool (ADHD)
18
0
Social Communication Questionnaire (SCQ) (autism)
40
0
PATHWAYS Gender Identity Questionnaire
0
2
Social Transition Questionnaire
0
5
Adolescent Primary Care Traumatic Stress Screen (APCTSS) (trauma screen)
5
5
Revised Child Anxiety and Depression Scale (RCADS) (anxiety and depression)
Body Image Scale – Gender Spectrum (BIS-GS) (body image)
0
33
Ask Suicide-Screening Questions (ASQ)
4
4
SCOFF Questionnaire – Test for Detecting Eating Disorders
5
5
Difficulties in Emotion Regulation Scale (DERS)
29
18
Sexual Attraction
0
1
ALSPAC Romantic Relations (sex life)
0
14
Parental Attitudes of Gender Expansiveness Scale for Youth (PAGES)
16
14
15 minutes questioning on ‘medical history’ that covers huge range of areas.
Unknown
Unknown
Annual Health Update
Unknown
Unknown
Total questions
Over 314 questions
Over 314 questions
Detailed Breakdown of the exact questions being asked
52 questions for parent & 52 questions for young person from the Kidscreen-52 tool (here the parent version)
In general how would your child rate their health? (excellent; very good; good; fair; poor)
Thinking about last week (with answers: not at all; slightly; moderately; very; extremely or never; seldom; quite often; very often; always)
Has your child felt fit and well
Has your child been physically active (e.g. running, climbing, biking)?
Has your child been able to run well?
Has your child felt full of energy
Has your child felt that life was enjoyable
Has your child felt pleased that they are alive
Has your child felt satisfied with their life
Has your child been in a good mood
Has your child felt cheerful
Has your child had fun
Has your child felt that they do everything badly
Has your child felt sad
Has your child felt so bad that they didn’t want to do anything
Has your child felt that everything in their life goes wrong
Has your child felt fed up
Has your child felt lonely
Has your child felt under pressure
Has your child felt happy with the way they are
Has your child been happy with their clothes
Has your child been happy with the way they look
Has your child felt jealous other the way other children look
Has your child wanted to change something about their body
Has your child had enough time for themselves
Has your child been able to do the things they want in their spare time
Has your child had enough opportunity to be outside
Has your child had enough opportunity to meet friends
Has your child been able to choose what to do in their free time
Has your child felt understood by their parents
Has your child felt loved by their parents
Has your child been happy at home
Has your child felt that their parents had enough time for them
Has your child felt that their parents treated them fairly
Has your child been able to talk to their parents when they wanted to
Has your child had enough money to do the same things as their friends
Has your child felt they had enough money for their expenses
Does your child feel they have enough money to do things with their friends
Has your child spent time with their friends
Has your child done things with other children
Has your child had fun with their friends
Has your child and their friends helped each other
Has your child been able to talk about everything with their friends
Has your child been able to rely on their friends
Has your child been happy at school
Has your child got on well at school
Has your child been satisfied with their teachers
Has your child been able to pay attention
Has your child been enjoying school
Has your child got along with their teachers
Has your child been afraid of other children
Have other children made fun of your child
Have other children bullied your child.
(the default questions use he/she and boys/girls language – I’m assuming they will adapt to use they and child as written above)
118 questions for parent & 118 questions for young person from the Child Behaviour Checklist
For each questions the available answers are:
0=Not true (as far as you know); 1=Somewhat or sometimes true; 2=Very true or often true
1.Acts too young for his/her age / I act too young for my age
2. Drinks alcohol without parent’s approval / I drink alcohol without my parent’s approval
3. Argues a lot / I argue a lot
4. Fails to finish things he/she starts / I fail to finish things I start
5. There is very little that he/she enjoys / There is very little that I enjoy
6. Bowel movements outside toilet / I like animals
7. Bragging, boasting / I brag
8. Can’t concentrate, can’t pay attention for long / I have trouble concentrating or paying attention
9. Can’t get their mind off certain thoughts/obsessions (describe) / I can’t get my mind off certain thoughts/obsessions (describe)
10. Can’t sit still, restless or hyperactive / I have trouble sitting still
11. Clings to adults or too dependent / I’m too dependent on adults
12. Complains of loneliness / I feel lonely
13. Confused or seems to be in a fog / I feel confused or in a fog
14. Cries a lot / I cry a lot
15. Cruel to animals / I am pretty honest
16. Cruelty, bullying or meanness to others / I am mean to others
17. Daydreams or gets lost in his/her thoughts / I daydream a lot
18. Deliberately harms self or attempts suicide / I deliberately try to hurt or kill myself
19. Demands a lot of attention / I try to get a lot of attention
20. Destroys his/her own things / I destroy my own things
21. Destroys things belonging to his/her family or others / I destroy things belonging to others
22. Disobedient at home / I disobey my parents
23.Disobedient at school / I disobey at school
24. Doesn’t eat well / I don’t eat as well as I should
25. Doesn’t get along with other kids / I don’t get along with other kids
26. Doesn’t seem to feel guilty after misbehaving / I don’t feel guilty after doing something I shouldn’t
27. Easily jealous / I am jealous of others
28. Breaks rules at home, school, or elsewhere / I breaks rules at home, school, or elsewhere
29. Fears certain animals, situations or places other than school / I am afraid of certain animals, situations or places other than school
30. Fears going to school / I am afraid of going to school
31. Fears he/she might think or do something bad / I’m afraid I might think or do something bad
32. Feels he/she must be perfect / I feel that I have to be perfect
33. Feels or complains that no one loves him/her / I feel that no one loves me
34. Feels others are out to get him/her / I feel that others are out to get me
35. Feels worthless or inferior / I feel worthless or inferior
36. Gets hurt a lot/accident prone / I accidently get hurt a lot
37. Gets in many fights / I get in many fights
38. Gets teased a lot / I get teased a lot
39. Hangs with others who get in trouble / I hang around with kids who get into trouble
40. Hears sound or voices that aren’t there / I hear sound or voices that other people think aren’t there
41.Impulsive or acts without thinking / I act without stopping to think
42. Would rather be alone than with others / I would rather be alone than with others
43. Lying or cheating / I lie or cheat
44. Bites fingernails / I bite my fingernails
45. Nervous, high-strung, or tense / I am nervous or tense
46. Nervous movements or twitching (describe) / parts of my body twitch or make nervous movements
47. Nightmares / I have nightmares
48. Not liked by other kids / I am not liked by other kids
49. Constipated, doesn’t move bowels / I can do certain things better than other kids
50. Too fearful or anxious / I am too fearful or anxious
51. Feels dizzy or lightheaded / I feel dizzy or lightheaded
52. Feels too guilty / I feel too guilty
53. Overeating / I eat too much
54. Over-tired, without good reason / I feel overtired without good reason
55. Overweight / I am overweight
56. Physical problems without known medical cause:
a) Aches or pains (not stomach or headache)
b) Headaches
c) Nausea, feels sick
d) Problems with eyes (not corrected by glasses)
e) Rashes or other skin problems
f) Stomach aches
g) Vomiting / throwing up
h) Other (describe)
57. Physically attacks people / I physically attack people
58. Picks nose/skin/other part of body (describe) / I picks my nose/skin/other part of body (describe)
59. Plays with own sex parts in public / I can be pretty friendly
60. Plays with own sex parts too much / I like to try new things
61. Poor school work / My school work is poor
62. Poorly coordinated or clumsy / I am poorly coordinated or clumsy
63. Prefers being with older kids / I would rather be with older kids than kids my own age
64. Prefers being with younger kids / I would rather be with younger kids than kids my own age
65. Refuses to talk / I refuse to talk
66. Repeats certain acts over and over; compulsions (describe) / I repeat certain acts over and over; compulsions (describe)
67. Runs away from home / I run away from home
68. Screams a lot / I scream a lot
69. Secretive, keeps things to self / I am secretive or keep things to myself
70. Sees things that aren’t there / I see things that other people think aren’t there
71. Self-conscious or easily embarrassed / I am self-conscious or easily embarrassed
72. Sets fires / I set fires
73. Sexual problems / I can work well with my hands
74. Showing off or clowning / I show off or clown
75. Too shy or timid / I am too timid or shy
76. Sleeps less than most kids / I sleep less than most kids
77. Sleeps more than most kids during day and/or night (describe) / I sleep more than most kids during day and/or night (describe)
78. Inattentive or easily distracted / I am inattentive or easily distracted
79. Speech problem (describe) / I have a speech problem (describe)
80. Stares blankly / I stand up for my rights
81. Steals at home / I steal at home
82. Steals outside the home / I steal from places outside the home
83. Stores up too many things they don’t need (describe) / I stores up too many things I don’t need (describe)
84. Strange behaviour (describe) / I do things other people think are strange
85. Strange ideas / I have thoughts other people would think are strange (describe)
86. Stubborn, sullen, or irritable / I am stubborn
87. Sudden changes in mood or feelings / My moods or feelings change suddenly
88. Sulks a lot / I enjoy being with people
89. Suspicious / I am suspicious
90. Swearing or obscene language / I swear or use dirty language
91. Talks about killing self / I think about killing myself
92. Talks or walks in sleep (describe) / I like to make others laugh
93. Talks too much / I talk too much
94. Teases a lot / I tease others a lot
95. Temper tantrums or hot temper / I have a hot temper
96. Thinks about sex too much / I think about sex too much
97. Threatens people / I threaten to hurt people
98. Thumb-sucking / I like to help others
99. Smokes, chews, or sniffs tobacco / I smokes, chew, or sniff tobacco
100. Trouble sleeping / I have trouble sleeping (describe)
101. Truancy or unexplained absence / I cut classes or skip school
102. Underactive, slow moving or lacks energy / I don’t have much energy
103. Unhappy, sad or depressed / I am unhappy, sad or depressed
104. Unusually loud / I am louder than other kids
105. Uses dugs/alcohol for nonmedical purposes / I use drugs for non-medical purposes
106. Vandalism / I like to be fair to others
107. Wets self during the day / I enjoy a good joke
108. Wets the bed / I like to take life easy
109. Whining / I try to help other people where I can
110. Wishes to be of opposite sex / I wish I were of the opposite sex
111. Withdrawn, doesn’t get involved with others / I keep from getting involved with others
112. Worries / I worry a lot
113. Please write in any problems your child has that were not listed above.
2 questions for parents on Parental ‘About Yourself’ Questionnaire
Do you identify’ as: ‘woman/girl’, ‘man/boy’, ‘transwoman/transgirl’, ‘transman/transboy’, ‘non-binary/genderqueer/agender/gender fluid’, ‘don’t know’, ‘prefer not to say’, ‘other’.
What was your sex assigned at birth? ‘female’, ‘male’, ‘don’t know’, and ‘prefer not to say’.
1. Is she/he now able to talk using short phrases or sentences? If no, skip to Question 8
2. Do you have a to-and-fro “conversation” with her/him that involves taking turns or building on what you have said
3. Does she/he ever use odd phrases or say the same thing over and over in almost exactly the same way (either phrases that she/he hears other people use or ones that she/he makes up).
4. Does she/he ever use socially inappropriate questions or statements? For example, does she/he regularly ask personal questions or make personal comments at awkward times
5. Does she/he ever get her/his pronouns mixed up (e.g. saying you or she/he for I).
6. Does she/he ever use words that she/he seems to have invented or made up herself/himself; put things in odd, indirect ways; or use metaphorical ways of saying things (e.g. saying hot rain for steam)
7. Does she/he ever say the same thing over and over in exactly the same way or insist that you say the same thing over and over again.
8. Does she/he ever have things that she/he seems to have to do in a very particular way or order or rituals that she/he insists that you go through
9. Does her/his facial expression usually seem appropriate to the particular situation, as far as you can tell
10. Does she/he ever use your hand like a tool or as if it were part of her/his own body (e.g. pointing with your finger, putting your hand on a doorknob to get you to open the door)#
11. Does she/he ever have any interests that preoccupy her/him and might seem odd to other people (e.g. traffic lights, drainpipes, timetables)
12. Does she/he ever seem to be more interested in parts of a toy or an object (e.g. spinning the wheels of a car), rather than in using the objects as it was intended.
13. Does she/he ever have any special interests that are unusual in their intensity but otherwise appropriate for her/his age and peer group (e.g. trains or dinosaurs)
14. Does she/he ever seem to be unusually interested in the sight, feel, sound, taste, or smell of things or people
15. Does she/he ever have any mannerisms or odd ways of moving her/his hands or fingers, such as flapping or moving her/his fingers in front of her/his eyes
16. Does she/he ever have any complicated movements of her/his whole body, such as spinning or repeatedly bouncing up and down.
17. Does she/he ever injure herself/himself deliberately, such as biting her/his arm or banging her/his head
18. Does she/he ever have any objects (other than a soft toy or comfort blanket) that she/he has to carry around
19. Does she/he ever have any particular friends or a best friend
20. Does she/he ever talk to you just to be friendly (rather than to get something)
21. Does she/he ever spontaneously copy you (or other people) or what you are doing (such as vacuuming, gardening, or mending things)
22. Does she/he ever spontaneously point at things around her/him just to show you things (not because she/he wants them)
23. Does she/he ever use gestures, other than pointing or pulling your hand, to let you know what she/he wants
24. Does she/he nod her/his head to indicate yes
25. Does she/he shake her/his head to indicate no
26. Does she/he usually look at you directly in the face when doing things with you or talking with you
27. Does she/he smile back if someone smiles at her/him
28. Does she/he ever show you things that interest her/him to engage your attention?
29. Does she/he ever offer to share things other than food with you
30. Does she/he ever seem to want you to join in her/his enjoyment of something
31. Does she/he ever try to comfort you if you are sad or hurt
32. If she/he wants something or wants help, does she/he look at you and use gestures with sounds or words to get your attention
33. Does she/he show a normal range of facial expressions
34. Does she/he ever spontaneously join in and try to copy the actions in social games, such as The Mulberry Bush or London Bridge Is Falling Down
35. Does she/he play any pretend or make-believe games
36. Does she/he seem interested in other children of approximately the same age whom she/he does not know
37. Does she/he respond positively when another child approaches her/him
38. If you come into a room and start talking to her/him without calling her/his name, does she/he usually look up and pay attention to you
39. Does she/he ever play imaginative games with another child in such a way that you can tell that each child understands what the other is pretending
40. Does she/he play cooperatively in games that need some form of joining in with a group of other children, such as hide-and-seek or ball games?
‘definitely a boy’, mainly a boy’, ‘in the middle’, ‘definitely a girl’, ‘mainly a girl’, ‘neither a boy or girl’, ‘not sure’ and ‘none of the above’.
2. Are there other words that you use to describe your gender identity? (select all that apply), ‘cisgender’, transgender’, ‘non-binary’, ‘agender’, ‘genderfluid’, ‘genderqueer’, ‘two-spirit’ and ‘other’.
“Have you socially transitioned in any of the following settings?”, followed by a checklist of five settings: Home, School, With Friends, Online, and Any Other Setting (e.g., holiday).
Children or parents rate how often symptoms occur, using a four-point scale: 0 (Never), 1 (Sometimes), 2 (Often), or 3 (Always).
The tool asks 25 different questions written for either a child to self-complete (the version below) or with slightly rephrased questions for an adult to complete (where question 1 is “My child worries about things”.
1. I feel sad or empty.
2. I worry when I think I have done poorly at something.
3. I would feel afraid of being on my own at home.
4. Nothing is much fun anymore.
5. I worry that something awful will happen to someone in my family.
6. I am afraid of being in crowded places (like shopping centers, the movies, buses, busy playgrounds).
7. I worry what other people think of me.
8. I have trouble sleeping.
9. I feel scared if I have to sleep on my own.
10. I have problems with my appetite.
11. I suddenly become dizzy or faint when there is no reason for this.
12. I have to do some things over and over again (like washing my hands, cleaning or putting things in a certain order).
13. I have no energy for things.
14. I suddenly start to tremble or shake when there is no reason for this.
15. I cannot think clearly.
16. I feel worthless.
17. I have to think of special thoughts (like numbers or words) to stop bad things from happening.
18. I think about death.
19. I feel like I don’t want to move.
20. I worry that I will suddenly get a scared feeling when there is nothing to be afraid of.
21. I am tired a lot.
22. I feel afraid that I will make a fool of myself in front of people.
23. I have to do some things in just the right way to stop bad things from happening.
Each questions asks: a) How happy are you with [insert name of a particular body part]?: With answers i) very happy ii) happy iii) neutral iv) unhappy v) very unhappy vi) don’t have.
Each question is followed up with: Would you want to change that body part if it was possible through medical or surgical treatment? i) Yes ii) No
This component is the least clear. It mentions covering the following vast topic areas that are defined as ‘Medical History’ Domains:
1. Family Context
2. Developmental History
3. Physical Health
4. Mental Health and Risk
5. Adverse childhood experiences
6. Safeguarding
7. Gender Development and Experiences
8. Sexual Development, Knowledge and Sexual Orientation
9. Education, Peer Relationships, and Social Context
10. Additional Information.
Clinical Judgements – Impact assessments and clinical evaluation for various aspects of the CYP’s development and wellbeing;
Parental Support – Judgements on the level of positive parental support and any conflicts between parents/carers/legal guardians or between parents/carers/legal guardians and the CYP.
Would be good to find out exactly what data is collected and why.
diagnoses including neurodevelopmental, mental health and physical health, received in the past year. number of GP appointments
planned surgeries or procedures
A&E attendances or other unplanned admissions in the past year.
The reasons for the GP appointments and A&E attendances
Length of hospital admission for planned surgeries or procedures and admissions following an A&E attendance
Experiences of therapeutic options
Data will also be collected on rates of referral to, uptake of and completion of:
Psychological therapy
Occupational therapy
Speech and language therapy,
Clinical nursing
Youth work support
School/College support
Non-endocrine pharmacological treatments
Compensation
Children/young people and parent/carer/legal guardian completing informant measures will each receive shop vouchers worth £20 for each data collection episode.
Last week Stonewall shared their latest strategy. Reading it you’d barely notice that trans children are facing an acute escalation in targeted persecution. Life is dire for trans kids in the UK right now. Here’s a very short list:
Healthcare – criminalised
Trans teens being medically detransitioned
Forced conversion practices disguised as therapy
Forced identity investigation
Social transition denied
Segregated and humiliated at school
Excluded from sports
Can’t even go on a school or DofE camping trip
Bullying and violence
Supportive families facing social services and police
Can’t change institutional records
No chance of protection from transphobic parents
Barred from trans positive social media connections
Fights to ban trans books from school and county libraries
Schools teaching transphobia
Lessons on the ‘sex-based right to be transphobic’
Transphobic and scientifically illiterate lessons on bodies and puberty
Ban on school resources about trans lives, esp for younger ages
No education for their peers on trans lives or trans rights
No action on transphobic bullying
Gov refuses to even recognise trans kids
From a policy angle, I can’t think how things can be worse? (don’t tell me how)
Stonewall’s strategy does not mention a crisis. It does not mention trans children facing the worst situation for their rights and wellbeing this century.
If you don’t even acknowledge the problem, how are we meant to believe you are a trusted ally in helping us solve it?
They describe their role as to be “pragmatic conveners”. I always worry when folks use the word pragmatic. It’s a bit like describing yourself as the sensible grownup in the room. It is often a way of talking down to those of us who ask for more, as though it is not possible to hold steadfast to certain principle and then act in pragmatic ways. Too often pragmatic is the word used to defend something else – selling out those who are less important to you.
“Turbulence” is another buzz word that Stonewall is using. It is a term that glosses over the reality that we are not all in the same boat, and this isn’t a bit of rocky weather, but a very clearly targeted and incredibly well funded attack on the weakest parts of our communities.
Our enemies are incredibly strategic and tenacious. Our ‘friends’ appear without strategy.
Stonewall – from foes to friends and back again?
Over a decade ago Stonewall was being protested for its transphobia.
In 2015 they chose to start working for trans people
In 2017 I critiqued their then strategy for failing to have anything to offer for trans children.
Under Nancy’s leadership they were suddenly reliable strong on advocating for trans children.
At the same time as Stonewall got better at sticking up for trans kids, they apparently lost political capital. Perhaps they stopped getting the ear of government. Perhaps they stopped being in the rooms of the powerful.
Does that mean that sticking up for trans kids was the wrong strategy?
Should trans kids be sacrificed in the name of political capital and influence?
Should advocacy for trans kids be blamed for Stonewall’s unpopularity amongst a media and political elite in the throngs of rampant transphobia?
Should advocacy for trans kids be blamed for being on the losing side of a culture war?
Would those culture warriors have bowed out and quit if Stonewall had been more pragmatic?
Consensus
The part of the strategy that really stuck in my throat is this sentence. “We will seek common ground and consensus”.
Billions of pounds have gone into the global anti-gender movement.
In the UK we have had 8 years of incessant misinformation, lies, propaganda and fearmongering about trans kids
Transphobic politicians created the illegitimate and prejudice riddled Cass Review that has greenlit all kind of persecution and discrimination against trans kids
Whole organisations have formed to advocate against trans kids rights. Organisations that are terrifying in their connections to those with power and funding.
Organisations fighting for trans kids rights have been weakened, have sold out, have been scared away
Public opinion has over the past 8 years got worse year after year on topics related to trans kids
We cannot get progress through common ground and consensus.
Common ground and consensus tells me that trans kids’ rights, trans kids’ lives are disposable, while you work on the areas where there is most consensus. Grow a bloody backbone.
An organisation standing up for trans rights, for trans kid’s rights at this point in history needs to be brave, needs to be principled, needs to proactively reshape the narrative through standing up clearly and articulately and strongly for trans kids’ rights at every turn.
We should be telling everyone who will listen that the current status quo is deeply harmful. That it is unfair. That it is persecuting trans kids just for being trans.
I don’t believe we will see change through consensus. We will see change through clearly putting our marker in the sand, and speaking up again and again and again, leading with our principles.
In the room where it happens
Those who talk of pragmatism and consensus want to be in the room where it happens. They want to have the ear of those in power.
Great for them.
But what message will they be saying in those powerful rooms?
Are they going to hold the government to account on all of its horrendous failings?
Or are they going to play polite, make a couple of challenging points on the less controversial issues, while letting a whole heap slide?
Are they going to bask in the warmth of the powerful while trans kids are out in the cold?
Do they even recognise how bad it is? Do we even trust that they care about all the above violence being pushed by our government onto trans children?
I’ve been in rooms with several leading (cis, white, male) LGBT sector leaders and they have said to my face (in politer terms) that they don’t support trans children. That they are not actually bothered by trans children’s rights violations. That trans children make them uncomfortable. That they are quite on the fence. That its all a bit much isn’t it. That rights for trans children is a step too far. Perhaps even that rights for trans children is harming the wider LGBT endeavour. Trans kids can wait for next century, their time is not now.
For those defending ‘pragmatism’, I am sometimes left to wonder if they are naïve to the real agenda, to the real lack of conviction amongst some leaders.
Is it pragmatism, or is it selling out trans kids entirely?
The good activist
Let’s also be honest here – there is not a shortage of organisations and individuals queueing up to the be ‘reasonable LGBT activists’ who are allowed into the rooms of the powerful.
But at what cost? If you sell out your weakest members to get into those rooms, to stay in those rooms?
Moving the needle
I don’t believe we are where we are due to lack of articulacy.
Or due to not being invited to play the token LGBT friend.
Or due to being too demanding.
I don’t think we have done anything wrong.
We have faced overwhelming power differentials, and have lost because of the scale of those power differentials.
Taking away a lesson that we just needed to do X or we just need to be politer or work more for slow progress or consensus, is learning the wrong lesson.
Being in the room isn’t going to shift the needle when the game is rigged. We certainly can’t win the consensus game in our current media landscape.
Winning through consensus, through playing nice, will take us decades.
And that isn’t winning at all really. It is giving up any chances for the current generation of trans kids. And for the one after. And the one after that.
What can we do?
I see three roles that stonewall can do in this current context:
Calling out persecution and injustice to embarrass those in power
This role is not nothing. There are parts of the Labour party who do not want to be known as the baddies. Most trans people view them as out and out baddies. Conveying this message to a wider public can embarrass Labour, and empower those in Labour who want to be less terrible.
2. Calling out persecution and injustice to embolden cis people
This is for me the biggest priority. There are a ton of cis people across the country working out how to respond to trans kids. Individual school teachers. GPs. Governors. Scouts leaders. Many will by default fall into the path of least resistance, which currently means following gov policy and guidance to harm trans kids. But clear messaging from stonewall on how unacceptable all of this is can embolden people to consider a different act. Most of life does not take place based on detailed following of government decree – it is in the small and everyday decisions and actions of millions of us. Having clear communication from Stonewall that the current government policy harms trans kids can turn the needle on those everyday decisions. Having clear communication from Stonewall that specific actions and policies are part of systemic persecution and genocidal intent (see recent statement from the Lemkin Institute), is something that we can give to individual school head teachers, to individual social workers, to individual family members, to legitimise the messages that we are currently trying to convey.
3. Calling out persecution and injustice to make us feel less alone
Even if nothing else, feeling that our current pain and fear is noticed, that we are not abandoned, that we have staunch allies – that actually matters. Even in the face of ongoing and perhaps not easy to fix persecution – it can help us take one more step – help us stay in the fight.
Today I saw photos of Stonewall smiling and celebrating at a 10 Downing Street ‘pride’ reception. I saw no public call outs of the horrific Labour policies that are destroying the chances of happiness for trans children across the UK. It felt a real kick in the teeth.
Finding Hope
The Stonewall strategy talks about being a “a beacon of hope”. I actually agree with this ambition. What does that hope look like? For me, I draw hope from knowing that organisations and individuals will be brave, will stand up and be counted, will call out oppression and persecution and ignorance and hate wherever they find it. This gives me hope. This can give hope to trans kids too – showing that their current atrocious treatment is noticed, showing that we recognise it for bigotry and violence, showing that we stand at their sides. The current Stonewall approach give me zero hope.
What they have given me, this evening, is rage. I am beyond done with sell outs and folks who are part of the problem. We have enough problems.
I know that Stonewall are not the real enemy. They are not the reason that life is so goddam hard. They are not the reason I am stressed and afraid.
I know that it is easy to turn on each other when we feel so powerless and defeated.
Maybe I should thank them for providing some rage.
Rage is more motivating than fear.
I just wish there were other things on the menu these days.
I keep coming across research, written by authors who are not non-binary, that includes the confident statement that a majority of non-binary people are not transgender, or that a majority of non-binary people are cisgender.
I will start by saying that identity is complex and personal and every individual can identify how they please. Naturally. Personally, I am trans and non-binary. I both identify as trans, and I also consider ‘trans’ as an umbrella term that has space underneath it to capture non-binary identities in general [whilst recognising that some non-binary people, just like some binary-oriented people of trans experience/history, don’t like to be called or recognise themselves as trans].
I personally feel stressed out and othered by language that defaults to ‘trans and non-binary people’ as though they are two distinct categories (I’m personally happier with a default assumption that the term trans will always include non-binary people, and where folks want to emphatically include non-binary people who reject trans as an umbrella I’m be ok with the cumbersome ‘trans and/or non-binary’. Of course humans are messy and no language will be perfect.
A conclusive and confident statement about a majority of non-binary people being cisgender always pushes me to ask the question – where is the data coming from?
In my personal experience, I’ve known many people who start out identifying as non-binary and ‘not trans’, who over time, embrace the umbrella label of trans [I’m not sure I’ve ever met anyone who has gone the other route]. I’ve known many non-binary people who initially feel that they cannot or must not take the label trans, that using such a label would be ‘appropriation’, if they have not medically transitioned enough, if they have not socially transitioned enough, if they have not suffered enough. With connections to trans communities I’ve known many such people come to adopt the label of trans. Whether an individual non-binary person finds meaning under the umbrella label trans is not a static binary and can change over time.
There is also a curious double standard in some surveys wherein non-binary people can be labelled as cis if they do not actively identify with the word trans, whereas trans is considered a default marker for binary-oriented trans people even if they do not personally identify with the term.
Lets look at the original report that is the root of the claim that a majority of non-binary people are cisgender and see whether there are any potential problems with that report.
It tells us confidently that “A greater percentage of nonbinary LGBTQ adults are cisgender rather than transgender”. I’ve seen this claim, that a majority of non-binary people are cisgender replicated in many publications.
There are several points to give us pause about the reliability of this claim.
Firstly the data comes from surveys conducted in the US in 2016-2018, that were designed in 2014. Identity language and knowledge amongst non-binary communities has been on a huge journey over the past decade. There are way more resources, groups and connections for non-binary people in 2025 than in 2016. Presuming that identity labels for non-binary people in the US in 2016 align with non-binary identity labels (worldwide!) in 2025 is a big assumption.
Secondly, the surveys from which this claim are drawn were not designed to find out whether non-binary people identify as trans, and were not designed, as far as I’m aware, in collaboration with non-binary authors. The summary report is from the Williams Institute, a research institute that has a history of being critiqued for some failings in the way it considers trans people’s data.
Take a look at this figure from the 2021 summary report and tell me if it might demonstrate some structural areas of ignorance or bias. As a non-binary reader this figure makes me dizzy. At best it begs some serious questions.
I tried to find out what was the underpinning data, what exact questions were people being asked in 2016 that led to the above diagram and it is rather complex and confusing.
The original sample comprised 1,369 LGB(T) people in 2016-2017 (people were asked if they were ‘lesbian, gay, bisexual, queer, or samegender loving’ and respondents needed to answer yes to be included).
On your original birth certificate was your sex assigned as male or female
Do you currently describe yourself as i) man, ii) woman or iii) transgender.
[In some versions of the survey a fourth option for part 2 was included “(iv) do not identify as female, male, or transgender”.]
Respondents who did not pick the option ‘transgender’ above were filtered into an LGB survey called the Generations study. It was presumed to be a study of cisgender people (though respondents were never asked if they identify as cisgender). (27 respondents who clicked man or woman rather than transgender in a way that did not match with their assigned sex were excluded from the Generations survey).
It is important to note that people only gain access to the Generations study if they click that their identity is ‘man’ or ‘woman’ in the initial filter question (making it harder to access, for say, non-binary people…).
The presumed cisgender participants of the Generations study are then asked about their gender identity:
“If you had to choose only one of the following terms, which best describes your current gender identity?” a) woman (744 answered this) b) man (665 answered this) c) non-binary/genderqueer (94 answered this). 15 did not respond.
Note none of these participants have been asked if they identify as cisgender, they are simply LGBT identifying participants who did not click on ‘transgender’ in the initial screening. These 94 people in the US are deemed to be ‘cisgender non-binary people’. This group of ‘non-binary/gender queer’ individuals are further sub-divided into those who are deemed ‘cisgender LB women’ and those who are deemed ‘cisgender GB men’ based on whether they had ticked man or woman in the very first question. All non-binary people must be a man or a woman.
People who clicked ‘transgender’ at the first question are steered to a separate survey called ‘transpop‘. Everyone in the second survey is classified as transgender, as they needed to specifically click the option ‘transgender’ for question one.
People in the transpop survey were asked about their ‘gender identity’.
They were asked two questions:
Which of the following terms best describes your gender identity? a) man, b) woman or c) genderqueer/non-binary.
Do you currently consider yourself a) man b) woman c) transgender.
If it seems that the questions options are confusing and non-logical, it is because they are confusing and non-logical.
Comparing the two surveys
1518 individuals completed phase one of the Generations survey, of whom 94 identified as non-binary. Only 274 people completed the transpop survey across all waves of that survey, of whom 76 identified as non-binary. The total number of those deemed cisgender non-binary men and cisgender non-binary women in the Generations survey (=96) was greater than the number of non-binary people in the transpop survey (=74). This leads to the confident conclusion that ‘a majority of non-binary people are cisgender. Despite not one non-binary person having been asked ‘are you cisgender’? Despite no questions that specifically recognise a non-binary person’s identity before asking whether the word transgender or trans as an identity term or an umbrella term is meaningful to them.
I do not find the above reliable or (globally) meaningful for providing insight into non-binary populations in 2025.
Overall
This survey from 2016-2017, designed in 2014, makes a range of questionable choices. I don’t think anyone would argue that these choices stand up in 2025 as a useful way of collecting information about trans and non-binary populations.
Most importantly, it never specifically asks non-binary people ‘do you identify as transgender yes or no’. ‘do you identify as cisgender yes or no’, or the question ‘do you feel comfortable defining your non-binary identity under a broader umbrella as trans’.
There are plenty of non-binary people who may not specifically identify with the word trans as a key self-descriptor, who nevertheless are happy under a broad ‘trans umbrella’.
It is a double standard to define all binary trans people as ‘trans’ based on e.g. identification as a man while having assigned gender female even if that individual does not personally ‘identify as’ trans, but limiting non-binary transness to only those who ‘identify as’ trans.
Overall I think identity and labels are messy, binaries are often false.
I do not think any of the above is a robust basis on which to make confident claims that ‘a majority of non-binary people are cisgender’.
Could we, maybe, actually ask non-binary people what we actually think?
Could we stop relying on surveys such as this deeply flawed 2021 Williams Institute survey for understanding non-binary lives?